Esta página é uma tradução gerada por IA do guia em inglês. Se você é falante nativo de português, ajude-nos a melhorar esta tradução usando o botão "Melhorar este guia" no final da página.
Segurança e interações medicamentosas
Quais medicamentos são perigosos de combinar com psilocibina, LSD ou 5-MeO-DALT, quem deve evitá-los e como minimizar riscos.
Essas substâncias são fisicamente muito seguras nas doses usadas para prevenção de cefaleia em salvas. Ao contrário de muitos medicamentos para cefaleia em salvas, elas não têm toxicidade conhecida em órgãos a longo prazo, não causam dependência e não provocam abstinência. Os principais riscos vêm de interações com outros medicamentos, de um pequeno número de condições preexistentes e de efeitos psicológicos se a dose for alta demais. Esta página cobre todos esses pontos em detalhe. Por favor, leia com atenção antes da sua primeira dose.
Checklist de segurança
Complete todos os itens desta lista antes da sua primeira dose.
- Medicamentos listados. Anotei todos os medicamentos, suplementos e fitoterápicos que tomo.
- Interações verificadas. Verifiquei cada um deles na tabela de medicamentos abaixo.
- Médico consultado (se necessário). Se for recomendado para os medicamentos que tomo (ver tabela), conversei com meu médico.
- Síndrome serotoninérgica compreendida. Entendo os sintomas e sei quando pedir ajuda.
- Acompanhante combinado. Tenho uma pessoa de confiança ciente do meu cronograma de doses, especialmente para a primeira dose.
- Período de eliminação de triptanos (se aplicável). Se eu tomo triptanos, vou esperar pelo menos cinco dias após a última dose antes de iniciar o protocolo.
Interações medicamentosas em resumo
Psilocibina, LSD e 5-MeO-DALT atuam todos no sistema serotoninérgico do cérebro. A serotonina é uma substância química que seu cérebro usa para regular humor, sono e dor. Muitos medicamentos comuns também agem nesse sistema. Quando dois ou mais fármacos afetam a serotonina ao mesmo tempo, seus efeitos podem se combinar de maneiras indesejadas: ou seja, podem desencadear uma condição chamada síndrome serotoninérgica.
Aqui está o resumo rápido:
- Lítio é uma contraindicação absoluta: não combine essas substâncias com lítio (risco de convulsão).
- Medicamentos e drogas serotoninérgicos (substâncias que agem no sistema da serotonina) exigem uma conversa com o médico. As duas categorias principais são:
- IMAOs. Risco médio-alto de síndrome serotoninérgica. Eles impedem o corpo de metabolizar triptaminas, intensificando e prolongando dramaticamente os efeitos.
- ISRSs e IRSNs. Risco médio-baixo de síndrome serotoninérgica. Também tendem a bloquear o funcionamento do protocolo e exigem um desmame longo antes de iniciar.
- Triptanos, ergotamínicos e muitos preventivos para cefaleia em salvas (verapamil, prednisona, topiramato, etc.) precisam ser interrompidos pelo menos cinco dias antes da primeira dose. Eles bloqueiam o funcionamento do protocolo.
- Tudo o mais: consulte seu médico.
Verifique seus medicamentos
Antes de iniciar o protocolo, faça uma lista de tudo o que você toma (medicamentos prescritos, medicamentos de venda livre, suplementos, fitoterápicos) e confira com esta tabela.
| Categoria | Nomes / exemplos | Risco | O que fazer |
|---|---|---|---|
| Lítio | Lithobid, Eskalith | Risco de convulsão: não combinar | Não há solução alternativa. O protocolo não é uma opção enquanto você estiver em uso de lítio. Converse com seu médico sobre fazer um desmame seguro caso queira tentar. |
| IMAOs | Fenelzina (Nardil), tranilcipromina (Parnate), isocarboxazida (Marplan), moclobemida (Manerix); antibiótico: linezolida; à base de plantas: chás de ayahuasca, arruda-síria, changa. | Médio-alto: risco de síndrome serotoninérgica + efeitos intensificados | É obrigatório conversar com seu médico. É obrigatório ter sempre um acompanhante presente. Leia a seção sobre síndrome serotoninérgica abaixo. |
| ISRSs / IRSNs | Fluoxetina (Prozac), sertralina (Zoloft), paroxetina (Paxil), citalopram (Celexa), escitalopram (Lexapro), venlafaxina (Effexor), duloxetina (Cymbalta), desvenlafaxina (Pristiq). | Médio-baixo: efeitos serotoninérgicos podem se somar; também bloqueia o protocolo | Converse com seu médico. ISRSs muitas vezes precisam ser reduzidos lentamente ao longo de semanas antes de iniciar. Nunca pare de tomar antidepressivos sem supervisão médica. |
| Triptanos | Sumatriptano (Imitrex), rizatriptano (Maxalt), zolmitriptano (Zomig), naratriptano (Amerge), frovatriptano (Frova), almotriptano (Axert), eletriptano (Relpax). | Risco serotoninérgico baixo; a principal preocupação é que eles bloqueiam o funcionamento do protocolo. | Espere pelo menos cinco dias após a última dose de triptano antes de iniciar o protocolo. Evite retomá-los durante o protocolo. |
| Ergotamínicos | Diidroergotamina (DHE), metisergida (Sansert), Cafergot, tartarato de ergotamina (Ergomar). | Bloqueiam o funcionamento do protocolo. | Interrompa pelo menos cinco dias antes da primeira dose. |
| Preventivos para cefaleia em salvas | Verapamil (Isoptin, Verelan, Calan), corticosteroides (prednisona, prednisolona, dexametasona), topiramato (Topamax), valproato de sódio (Depakote), carbamazepina (Tegretol). | Bloqueiam o funcionamento do protocolo. | Converse com seu médico sobre interromper com segurança. Alguns precisam de desmame. Espere pelo menos cinco dias após a interrupção antes da primeira dose. |
| Outras drogas serotoninérgicas | Antidepressivos tricíclicos (amitriptilina, nortriptilina, imipramina, clomipramina), opioides (tramadol, metadona, fentanil, hidrocodona, oxicodona), dextrometorfano (em muitos xaropes para tosse), erva-de-São-João, anfetaminas (Adderall, Vyvanse), MDMA / ecstasy. | Variável: depende da combinação | Converse com seu médico. Vários medicamentos serotoninérgicos tomados juntos podem se somar até um risco significativo, mesmo que cada um deles isoladamente pareça seguro. |
| Álcool e nicotina | Cerveja, vinho, destilados; cigarros, charutos, fumo de mascar, rapé. | Baixo (não é serotoninérgico); no entanto, ambos são gatilhos conhecidos de cefaleia em salvas. | Evite nos dias de dosagem e no dia seguinte. Muitos pacientes com cefaleia em salvas evitam totalmente durante um ciclo. |
Se seu medicamento não estiver nesta lista, não presuma que ele seja seguro. Pesquise o nome do seu medicamento mais "serotonina" na internet, ou pergunte ao seu médico ou farmacêutico.
Como conversar com seu médico
Muitos médicos têm conhecimento limitado sobre tratamentos assistidos por psicodélicos, e você pode temer ser julgado. Aqui está uma abordagem sugerida:
-
Apresente como redução de danos. "Tenho cefaleia em salvas e venho lendo sobre pessoas que usam pequenas doses de psilocibina (ou LSD, ou 5-MeO-DALT) para prevenir os ataques. Eu gostaria da sua ajuda para garantir que seja seguro com meus medicamentos."
-
Leve esta página. Mostre a eles a tabela de medicamentos acima e a seção sobre síndrome serotoninérgica abaixo. Médicos respondem bem a perguntas específicas e concretas.
-
Pergunte sobre seus medicamentos específicos. "Você pode verificar se algum dos meus medicamentos prescritos interage com um agonista de receptor de serotonina?"
-
Saiba que eles não podem denunciá-lo. Conversas entre médico e paciente são confidenciais. Seu médico pode aconselhar contra, mas não pode denunciá-lo às autoridades por perguntar.
-
Se seu médico se recusar a conversar, isso é um sinal para buscar outra opinião, se possível. Alguns neurologistas, especialistas em cefaleia e psiquiatras conhecem a prática dos pacientes e podem orientar sobre o uso seguro.
Síndrome serotoninérgica: o que você precisa saber
A síndrome serotoninérgica acontece quando seu cérebro fica inundado de serotonina em excesso. É mais provável quando uma dessas substâncias é combinada com outro fármaco que também eleva a serotonina, especialmente IMAOs, ou com múltiplos fármacos serotoninérgicos se somando. Ela é tratável, e conhecer os sinais é o que torna a situação manejável, e não perigosa.
O risco aumenta com doses maiores e com mais medicamentos serotoninérgicos, mas é difícil prever de antemão exatamente qual combinação ou dose vai desencadeá-la. É por isso que recomendamos conversar com seu médico, começar com doses baixas e ter um acompanhante.
Sintomas
Chame o serviço de emergência imediatamente se ocorrer qualquer um destes sintomas graves:
- Convulsão (tremores incontroláveis, perda de consciência).
- Febre alta (acima de 38,5°C / 101,3°F).
- Desmaio.
- Espasmos musculares graves ou rigidez muscular (seu corpo parece travado).
- Movimentos oculares laterais incontroláveis.
- Batimento cardíaco rápido ou irregular combinado com sensação de mal-estar intenso.
- Qualquer sintoma (incluindo os mais leves abaixo) que piore rapidamente.
Chame seu médico se você apresentar estes sintomas mais leves:
- Batimento cardíaco acelerado, calafrios ou sudorese intensa persistindo após 30 minutos.
- Contrações ou espasmos musculares.
- Náusea ou diarreia.
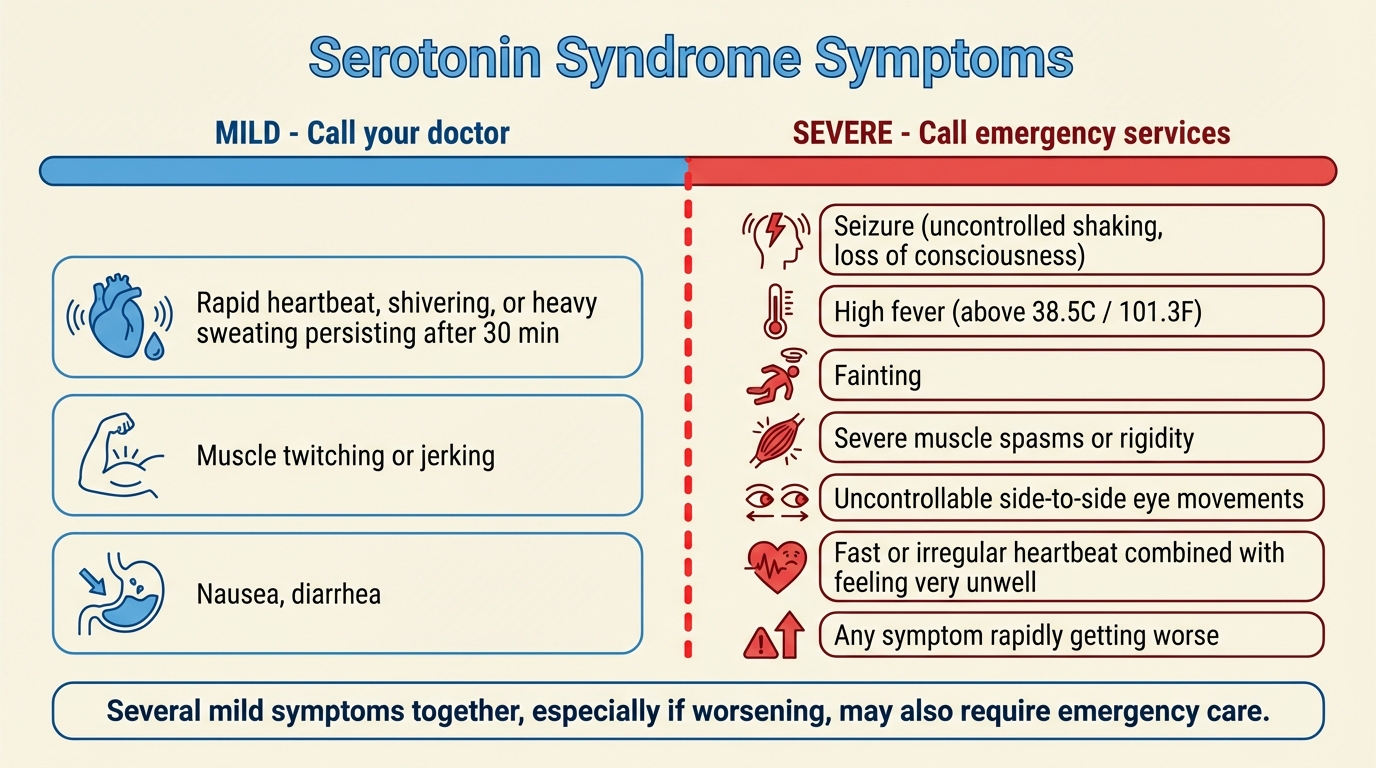
Os sintomas da síndrome serotoninérgica vão de leves (à esquerda) a graves (à direita). A linha vermelha marca o momento de chamar o serviço de emergência.
Se em algum momento você precisar de atendimento médico de emergência, é fundamental que a equipe médica saiba o que você tomou. Diga a eles que você tomou psilocibina (ou LSD, ou 5-MeO-DALT) e liste todos os outros medicamentos. A síndrome serotoninérgica é tratável, mas precisa ser corretamente identificada.
Recursos para mais detalhes
- Demystifying Serotonin Syndrome (Canadian Family Physician) — inclui uma ficha informativa para o paciente que pode ser impressa.
- Serotonin Syndrome (Cleveland Clinic).
- Serotonin Syndrome (Mayo Clinic).
Interações medicamentosas em detalhe
Esta seção explica cada categoria de medicamento da tabela acima com mais profundidade. Leia as partes que se aplicam a você.
Lítio
O lítio é um estabilizador de humor prescrito para transtorno bipolar e também usado como tratamento preventivo para cefaleia em salvas. A combinação de lítio com psilocibina ou LSD pode causar convulsões. A evidência mais direta é uma análise da Johns Hopkins de 2021 sobre relatos de experiência publicados online: de 62 relatos descrevendo a combinação de um psicodélico clássico com lítio, 47% envolveram convulsões e 39% envolveram uma visita ao atendimento médico. Em contraste, 0 de 34 relatos de psicodélicos combinados com lamotrigina (um estabilizador de humor diferente) envolveram convulsões.[2] O mecanismo não é totalmente compreendido, e não há dados específicos sobre o 5-MeO-DALT, mas a suposição prudente é que o mesmo risco se aplica.
Se você toma lítio, não inicie este protocolo. Converse com seu médico sobre fazer um desmame seguro se quiser tentar. O lítio tem uma janela terapêutica estreita e precisa ser reduzido lentamente sob supervisão médica.
IMAOs
IMAOs (inibidores da monoamina oxidase) são medicamentos que retardam a capacidade do corpo de metabolizar serotonina e triptaminas. Isso cria duas preocupações distintas quando combinados com psilocibina ou 5-MeO-DALT (o LSD é metabolizado por uma via diferente e é menos afetado, mas ainda assim cabe cautela):
- Síndrome serotoninérgica. Como os IMAOs impedem o corpo de eliminar a serotonina normalmente, ela pode se acumular a níveis perigosos. Os sintomas podem se desenvolver durante ou mesmo horas após a tomada da dose. Veja a seção sobre síndrome serotoninérgica acima.
- Efeitos intensificados e prolongados. IMAOs tornam as triptaminas ativas por via oral dramaticamente mais fortes e mais duradouras. Uma dose que normalmente produziria efeitos preventivos leves pode, em vez disso, produzir uma experiência psicodélica intensa.
IMAOs comuns incluem:
- Antidepressivos prescritos: fenelzina (Nardil), tranilcipromina (Parnate), isocarboxazida (Marplan), moclobemida (Manerix).
- Antibióticos: linezolida.
- À base de plantas: chás de ayahuasca, arruda-síria (harmal), misturas de changa (que frequentemente contêm harmina ou harmalina).
Se você toma um IMAO, é obrigatório conversar com seu médico antes de iniciar. Se seu médico der aval, sempre tenha um acompanhante que conheça os sintomas da síndrome serotoninérgica e peça para ele ficar com você por pelo menos uma hora depois. Os sintomas podem ser retardados quando há IMAOs envolvidos.
ISRSs e IRSNs
ISRSs e IRSNs são antidepressivos muito comumente prescritos. Eles atuam aumentando os níveis de serotonina no cérebro. Quando combinados com psilocibina, LSD ou 5-MeO-DALT (que também ativam receptores de serotonina), há duas questões:
- Soma de efeitos serotoninérgicos. O risco de síndrome serotoninérgica a partir de uma pequena dose preventiva combinada com um único ISRS ou IRSN é geralmente considerado baixo, mas não é zero, especialmente se você também toma outros medicamentos que afetam a serotonina.
- Bloqueio do protocolo. ISRSs e IRSNs também estão entre os bloqueadores mais confiáveis dessas substâncias. Pacientes em uso de ISRSs frequentemente descobrem que o protocolo simplesmente não funciona até que o ISRS tenha saído do organismo.
ISRSs comuns: citalopram (Celexa), escitalopram (Lexapro), fluoxetina (Prozac), fluvoxamina (Luvox), paroxetina (Paxil), sertralina (Zoloft).
IRSNs comuns: venlafaxina (Effexor), duloxetina (Cymbalta), desvenlafaxina (Pristiq).
Converse com seu médico antes de combinar o protocolo com qualquer ISRS ou IRSN. Tenha um acompanhante durante suas primeiras doses e certifique-se de que ele esteja familiarizado com os sintomas da síndrome serotoninérgica.
Triptanos
Triptanos (sumatriptano, etc.) são comumente usados para abortar ataques de cefaleia em salvas. Há duas preocupações:
- Bloqueio do protocolo. Esta é a preocupação maior para a prevenção. Triptanos estão entre os bloqueadores mais confiáveis. Pacientes que continuam usando triptanos durante o protocolo geralmente descobrem que ele não funciona.
- Síndrome serotoninérgica. Triptanos interagem com o sistema serotoninérgico, mas as evidências atuais sugerem que é improvável que contribuam significativamente para a síndrome serotoninérgica. Ainda assim, cautela é recomendada, especialmente se você toma outros medicamentos serotoninérgicos.
Recomendação: Espere pelo menos cinco dias após sua última dose de triptano antes de iniciar o protocolo. Exceção: frovatriptano (Frova) tem meia-vida mais longa, então espere pelo menos sete dias. Muitos pacientes descobrem que, uma vez que o protocolo funcione, precisam de triptanos com muito menos frequência.
Outras drogas serotoninérgicas
Muitos medicamentos comuns afetam a serotonina, mesmo que esse não seja seu propósito principal. Isoladamente, a maioria deles tem baixo risco de interação. Mas vários medicamentos serotoninérgicos tomados juntos podem se somar até um risco significativo, mesmo que cada um isoladamente pareça seguro.
Os medicamentos nessa categoria incluem:
- Antidepressivos tricíclicos (ADTs): clomipramina, imipramina, amitriptilina, nortriptilina.
- Analgésicos opioides: tramadol, metadona, meperidina, fentanil. Observação: a morfina não tem interação serotoninérgica perigosa.
- Antitussígeno: dextrometorfano (DXM), encontrado em medicamentos de venda livre para resfriado e tosse.
- Fitoterápicos: erva-de-São-João, um suplemento herbal comum para humor.
- Estimulantes: anfetamina (Adderall, Vyvanse).
- Drogas recreativas: MDMA / ecstasy.
- Anti-histamínicos: clorfeniramina, bromfeniramina.
Álcool e nicotina
Álcool e tabaco são gatilhos conhecidos para ataques de cefaleia em salvas durante um ciclo. A maioria dos pacientes já os evita. Além disso, há duas razões específicas para evitá-los nas proximidades das doses:
- Evite álcool nos dias de dosagem e no dia seguinte. Ele pode intensificar a experiência de forma imprevisível e pode interferir no protocolo.
- Evite uso intenso de tabaco durante a dose. Alguns pacientes relatam que a náusea piora com a nicotina.
Uma observação sobre opiáceos
A inclusão dos opiáceos na lista de bloqueadores vem da lista da comunidade de pacientes do Clusterbusters,[1] baseada na experiência acumulada de que eles podem atenuar o efeito do protocolo. A base farmacológica é menos bem estabelecida do que para as outras categorias acima, mas um pequeno conjunto de pesquisas antigas com animais mostrou que opioides e psicodélicos serotoninérgicos podem interagir no nível dos receptores, com opioides antagonizando efeitos alucinógenos em doses baixas.[3] Os pacientes são aconselhados a pecar pela prudência e interromper ou reduzir os opiáceos vários dias antes da dosagem, em coordenação com o médico prescritor.
Medicamentos geralmente considerados seguros
Os seguintes não são conhecidos por interagir significativamente com essas substâncias:[1]
- Antibióticos (com exceção da linezolida, ver IMAOs).
- AINEs (anti-inflamatórios não esteroidais): aspirina, acetaminofeno / paracetamol, ibuprofeno, naproxeno, indometacina.
- Antiácidos e medicamentos antiulcerosos.
- Medicamentos para asma.
- Insulina.
- Cafeína e bebidas energéticas.
- Complexo B e multivitamínicos.
- A maioria dos medicamentos para pressão arterial (por exemplo, Diovan), embora você deva conversar com seu médico se tiver preocupações cardiovasculares.
- Estatinas (por exemplo, Lipitor).
- Antieméticos (meclizina, dimenidrinato).
Essa lista não é exaustiva. Se você toma um medicamento que não está mencionado aqui, pesquise ou pergunte a um médico bem informado antes de prosseguir.
Quem NÃO deve usar essas substâncias
Gravidez
Não tome psilocibina, LSD ou 5-MeO-DALT se estiver grávida, tentando engravidar ou amamentando. Compostos triptamínicos podem causar contrações uterinas e podem representar riscos para o feto em desenvolvimento.
História pessoal ou familiar de psicose
Nessas doses baixas, essas substâncias podem, raramente, desencadear ou piorar episódios psicóticos. Pacientes diagnosticados com transtorno psicótico, ou cujos pais ou irmãos biológicos tenham sido diagnosticados, são aconselhados a não tomar nenhuma dessas substâncias. Transtornos psicóticos incluem esquizofrenia, transtorno esquizoafetivo, transtorno delirante e formas graves de alguns transtornos de humor. Uma grande meta-análise constatou que a incidência de psicose induzida por psicodélicos é de aproximadamente 0,002% em estudos populacionais.[4]
História pessoal ou familiar de transtorno bipolar
O transtorno bipolar é um caso especial. A maioria dos estudos clínicos modernos com psilocibina excluiu tanto pessoas com transtorno bipolar quanto pessoas com parentes de primeiro grau (pais, irmãos, filhos) que o têm. A preocupação é que os psicodélicos possam, raramente, desencadear um episódio maníaco ou psicótico em alguém com predisposição genética. Uma revisão de 2024 das evidências disponíveis concluiu que o risco varia dependendo de fatores como qual tipo de bipolar há na família, quão próximo é o parente e a própria idade do paciente, e propôs uma abordagem mais matizada do que a exclusão generalizada.[5] O resumo honesto é: o risco é real, mas provavelmente pequeno para a maioria das pessoas nessa categoria, e difícil de quantificar com precisão.
Se transtorno bipolar é frequente em sua família imediata, por favor, discuta isso com um psiquiatra antes de considerar o protocolo. Se você mesmo tem transtorno bipolar, o risco é significativamente maior e recomendamos não usar essas substâncias.
Cardiopatias, pressão alta ou histórico de AVC
Triptaminas e lisergamidas causam um aumento pequeno e temporário na frequência cardíaca e na pressão arterial durante a dose, semelhante ao exercício leve. Para a maioria das pessoas, isso é inofensivo. Se você tem uma cardiopatia grave, pressão alta não controlada, histórico de AVC ou problemas circulatórios significativos, converse com seu médico antes de prosseguir.
Doença hepática
Psilocibina, LSD e 5-MeO-DALT são processados pelo fígado. Se você tem doença hepática significativa, converse com seu médico primeiro.
Set e setting
"Set e setting" é o termo usado para descrever seu estado mental ("set") e seu ambiente físico ("setting") no momento da dose. Ambos podem moldar como a experiência vai transcorrer. Mesmo nas pequenas doses preventivas usadas aqui, onde os efeitos psicoativos costumam ser leves, set e setting importam.
- Evite tomar a dose durante uma crise emocional. Tomar essas substâncias durante ou logo após um evento emocional importante (uma separação, uma morte, uma discussão séria) pode amplificar esses sentimentos de formas que não ajudam. Se algo pesado está acontecendo na sua vida, adie a dose por alguns dias, se puder.
- Escolha um lugar calmo e familiar. Sua casa geralmente é a melhor opção. Iluminação suave, uma poltrona ou sofá confortável, água, música e um lanche ao alcance.
- Tenha uma pessoa sóbria e de confiança ciente do seu cronograma de doses. Especialmente na primeira vez, alguém em quem você confie deve saber o que você está fazendo e estar acessível.
- Não dirija, não opere maquinário e não tome decisões importantes durante a dose. Isso vale por toda a duração dos efeitos, que pode ser de 8 horas ou mais para o LSD.
Efeitos colaterais comuns
Nas pequenas doses usadas para prevenção, os efeitos colaterais costumam ser leves e duram apenas enquanto a dose está ativa.
Psilocibina e LSD
- Náusea leve na primeira hora.
- Leve calor corporal ou "body buzz".
- Elevação do humor ou risadinhas.
- Leve sensibilidade ao som ou à luz.
- Mudanças visuais ou sensoriais sutis.
- Frequência cardíaca ligeiramente elevada.
- Aumento da emotividade.
5-MeO-DALT
- Redução da temperatura corporal, dedos das mãos e dos pés frios (o efeito colateral mais comum, em 41% dos participantes da pesquisa).[6]
- Tontura ou náusea leves (22%).
- Sonolência acentuada e relaxamento intenso.
- 33% dos participantes da pesquisa não relataram nenhum efeito colateral.
Efeitos colaterais de uma dose maior (por exemplo, 25 mg ou mais de DALT, ou mais de 1 g de cogumelos) tendem a ser versões mais fortes dos mesmos. Permaneça nas doses baixas descritas no protocolo, a menos que você tenha um motivo específico para aumentar.
Quando interromper e procurar atendimento médico
Procure atendimento médico se você apresentar qualquer um dos seguintes:
- Dor no peito, falta de ar grave ou sinais de AVC (fala arrastada, fraqueza súbita de um lado).
- Uma convulsão.
- Confusão grave que não se resolve à medida que a dose passa.
- Um rompimento claro com a realidade (ouvir vozes, delírio profundo) que persiste além da duração da dose.
- Sintomas de síndrome serotoninérgica que sejam graves ou que estejam piorando.
- Pensamentos suicidas que pareçam fora do seu controle.
A cefaleia em salvas em si está associada a uma alta taxa de ideação suicida, e às vezes é chamada de "cefaleia do suicídio" por essa razão. Se você está tendo esses pensamentos em algum momento, seja durante o protocolo ou não, por favor, procure uma linha de crise, uma pessoa de confiança ou seu médico.
References
- ↩ Clusterbusters (2024). Alternative Treatments. Clusterbusters. Link
- ↩ Nayak SM, Gukasyan N, Barrett FS, Erowid E, Erowid F, Griffiths RR (2021). Classic psychedelic coadministration with lithium, but not lamotrigine, is associated with seizures: an analysis of online psychedelic experience reports. Pharmacopsychiatry, 54(5), 240–245. doi:10.1055/a-1524-2794
- ↩ Glennon RA (1986). Opioid-hallucinogen interactions. Pharmacology Biochemistry and Behavior, 24(6), 1655–1665. Link
- ↩ Sabé M, Sulstarova A, Glangetas A, De Pieri M, Mallet L, Curtis L, et al. (2025). Reconsidering evidence for psychedelic-induced psychosis: An overview of reviews, a systematic review, and meta-analysis of human studies. Molecular Psychiatry, 30(3), 1223–1255. doi:10.1038/s41380-024-02800-5
- ↩ Downey AE, Bradley ER, Lerche AS, O'Donovan A, Krystal AD, Woolley J (2024). A plea for nuance: should people with a family history of bipolar disorder be excluded from clinical trials of psilocybin therapy?. Psychedelic Medicine, 2(2), 61–70. doi:10.1089/psymed.2023.0051
- ↩ Post M (2015). Cluster headache patient survey: 5-MeO-DALT. Self-published.
Esta página foi útil para você?
Isenção de Responsabilidade
As informações deste site são fornecidas apenas para fins educacionais e de redução de danos. Elas não constituem aconselhamento médico e não devem substituir a consulta com um profissional de saúde qualificado. Consulte nossa página Aviso Legal para mais detalhes.