Prevenir ataques de cefalea en racimos con psilocibina, LSD y 5-MeO-DALT
Explicamos los fundamentos de la psilocibina, el LSD y la 5-MeO-DALT, y cómo utilizarlos de forma segura para prevenir ataque de cefalea en racimos.
For many patients, psilocybin, LSD, and 5-MeO-DALT are the most effective preventive treatments for cluster headaches available. They act pharmacologically in very similar ways and are somewhat chemically similar, and patients use them with the same simple protocol. Used carefully, they can significantly reduce, and sometimes completely stop, cluster headache attacks. This guide explains what each substance is, what the science says about them, and how to use them safely.
A small dose every few days can break a cluster cycle
For nearly 30 years, patients have known that a small dose of psilocybin (the active ingredient in "magic mushrooms") or LSD, taken every few days, can stop cluster cycles in their tracks. Since around 2015, patients have been finding the same with 5-MeO-DALT, a lesser-known compound that works similarly well. Many have been using these substances successfully for years, and for some they are the only treatment that works.
This guide was written for you: someone in serious pain, perhaps unfamiliar with psychedelics, looking for clear and comprehensive information. No prior experience is assumed. We will explain what these substances look like and how to take them safely.
These substances do not work for everyone, and they are illegal in most countries (with 5-MeO-DALT being the main exception). They are not meant for stopping an attack that has already started. For that, inhaling high-flow oxygen or vaporized DMT works much better. But for prevention, they are one of the most powerful tools patients have.
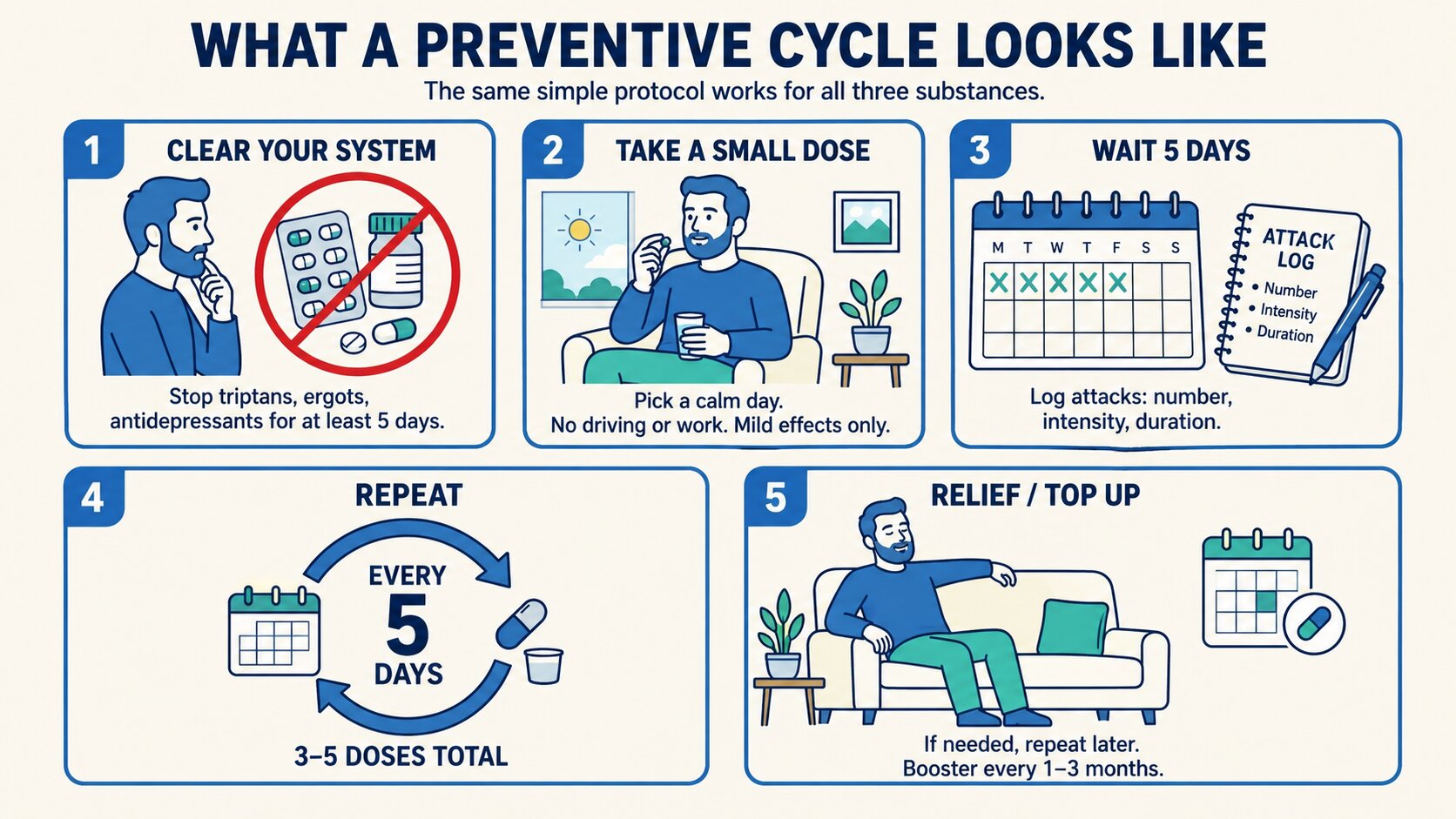
What a preventive cycle looks like
The same simple protocol works for all three substances.
Here is the protocol at a glance. The details vary slightly between substances (covered in the full chapters), but the overall shape is the same.
-
Clear your system. Stop other cluster medications (especially triptans, ergots, and antidepressants) for at least five days. These can block the treatment.
-
Take a small dose. Pick a calm day with no driving or work. Take a modest dose, small enough that the psychedelic effects are mild. Sit somewhere quiet for a few hours.
-
Wait about five days. If you are in a cluster cycle, keep a simple log of your attacks: how many, how intense, how long.
-
Repeat. Take another small dose every five days, for three to five doses total, or until the cycle breaks.
-
Top up when needed. If the cycle returns, repeat the process. Many patients also take a single "booster" dose every one to three months as maintenance.
Most people who respond start to notice an effect within the first one to three doses: fewer attacks, shorter attacks, or longer pain-free periods. Some break the cycle in a week, others need a couple of rounds.
Three substances, one protocol
You only need one of these three substances. Pick whichever you can obtain safely with minimal legal risk in your situation. Patients choose based on availability, cost, legality, and personal preference. Results tend to be similar across all three, but each has its pros and cons.
Psilocybin (magic mushrooms)
The most widely used option, and the one with the most clinical research behind it. Psilocybin is the active compound in certain species of mushroom, most commonly Psilocybe cubensis. Patients typically eat a small amount of dried mushrooms, around half a gram, which produces mild effects for 4–6 hours. Mushrooms can be grown at home fairly easily and cheaply, which makes psilocybin the most accessible option for many patients. It is illegal in most countries, though enforcement for personal medical use is usually low or decriminalized in some countries and cities.
LSD
LSD is potent and usually administered on a small piece of blotter paper or a drop of liquid. It has been used for decades to prevent cluster headache and is as effective, if not more effective, than psilocybin in patients' reports. The dose used is small, around 25–50 micrograms. The main drawback is that its full effects last longer (8 to 12 hours at recreational doses, less at the small preventive doses used here), and it is harder for most patients to source reliably. It is illegal in most countries.
5-MeO-DALT
5-MeO-DALT, sometimes just called "DALT", is the option you may not have heard of. It is a synthetic tryptamine, closely related to the other two, that patients have been using successfully since around 2015. At the doses used for prevention (typically 10 to 20 milligrams), it produces almost no hallucinogenic effects, just a mild body feeling for a couple of hours. It is also still legal in most countries, which makes it uniquely accessible. The tradeoff is that it is newer, less well-known, and has very little formal clinical research behind it; the evidence is mostly patient testimonials and two self-published patient surveys. For many patients, the combination of effectiveness, mildness, and legality makes it the preferred option once they hear about it.
What the science says
Patients have been using psilocybin and LSD to prevent cluster headaches since the late 1990s, and 5-MeO-DALT since around 2015. The formal medical research is still catching up, but the picture from the studies that do exist is consistent and encouraging.
Patient surveys. In 2006, a team at Harvard published the first peer-reviewed survey of cluster headache patients using these substances.[1] Of 53 patients, 22 of 26 said psilocybin aborted attacks; about half of psilocybin users and seven of eight LSD users said it ended their cluster period; and 18 of 19 psilocybin users and four of five LSD users said it extended their pain-free remission. A larger Clusterbusters survey in 2015, with 496 participants, found that psilocybin, LSD, and a related compound (LSA) were rated as comparable to or more effective than most conventional medications, and uniquely able to shorten or end a cluster cycle.[2] Surveys from the Netherlands, Italy, and Sweden have all found similar patterns: when patients use these substances, they tend to rate them as the most effective option they have tried.[3][4][5]
Clinical trials of psilocybin. In 2022, researchers at Yale published the first randomized controlled trial of psilocybin for cluster headache.[6] They gave a small group of patients three low doses, five days apart. The reduction in attack frequency did not reach statistical significance in this small sample, but the effect was strongest in chronic patients (a large effect size that lasted the full eight weeks measured). A blinded extension trial published in 2024 showed that when patients returned for a second round of psilocybin, attack frequency dropped by about 50%, a statistically significant result.[7] A separate Danish study in 2024 also found psilocybin reduced attacks by about 31% in chronic patients, and used brain imaging to suggest that the benefit may involve changes in the hypothalamus, the brain region thought to drive cluster headaches.[8] A small Swiss case series in 2025 reported that eight of nine treatment-resistant patients responded positively to psilocybin or LSD.[9]
Evidence for 5-MeO-DALT. Formal research on 5-MeO-DALT is much thinner. The two main sources are a 2014 case study and a 2015 patient survey, both by Mitchell Post. In the case study, two refractory chronic patients achieved complete relief at 15 mg every five days.[10] In the follow-up survey of 46 diagnosed cluster headache patients, 87% reported a reduction in their cluster headaches, with 61% experiencing a dramatic decrease or complete elimination of attack frequency, and 46% reporting zero attacks following treatment.[11] The evidence base is small, but the effect sizes reported are striking.
A recent narrative review covering all current and novel cluster headache therapies concludes that psilocybin and LSD show real promise based on case series, surveys, and the early trials, with serotonin 5-HT2A receptor activity as the suspected mechanism.[12] More research is needed, but the existing evidence is strong enough that several major academic centres now run cluster headache trials of these substances.
In short: these are not miracle cures, and the formal evidence base is still building. But the consistency between patient reports, surveys, and the early trials is a strong indicator, and is part of why a growing number of neurologists now take this approach seriously.
Hear from patients

Tommy Young, chronic cluster headache patient
References
- ↩ Sewell RA, Halpern JH, Pope HG Jr (2006). Response of cluster headache to psilocybin and LSD. Neurology, 66(12), 1920–1922. doi:10.1212/01.wnl.0000219761.05466.43
- ↩ Schindler EAD, Gottschalk CH, Weil MJ, Shapiro RE, Wright DA, Sewell RA (2015). Indoleamine hallucinogens in cluster headache: Results of the Clusterbusters Medication Use Survey. Journal of Psychoactive Drugs, 47(5), 372–381. doi:10.1080/02791072.2015.1107664
- ↩ Di Lorenzo C, Coppola G, Di Lorenzo G, et al. (2016). The use of illicit drugs as self-medication in the treatment of cluster headache: results from an Italian online survey. Cephalalgia, 36(2), 194–198.
- ↩ de Coo IF, Naber WC, Wilbrink LA, et al. (2019). Increased use of illicit drugs in a Dutch cluster headache population. Cephalalgia, 39(5), 626–634.
- ↩ Smedfors G, Liljenberg T, Steinberg A (2024). Use of prescribed and non-prescribed treatments for cluster headache in a Swedish cohort. Cephalalgia.
- ↩ Schindler EAD, Sewell RA, Gottschalk CH, et al. (2022). Exploratory investigation of a patient-informed low-dose psilocybin pulse regimen in the suppression of cluster headache: results from a randomized, double-blind, placebo-controlled trial. Headache, 62(10), 1383–1394. doi:10.1111/head.14420
- ↩ Schindler EAD, Sewell RA, Gottschalk CH, Flynn LT, Zhu Y, Pittman BP, et al. (2024). Psilocybin pulse regimen reduces cluster headache attack frequency in the blinded extension phase of a randomized controlled trial. Journal of the Neurological Sciences, 460, 122993. doi:10.1016/j.jns.2024.122993
- ↩ Madsen MK, Petersen AS, Stenbæk DS, et al. (2024). CCH attack frequency reduction after psilocybin correlates with hypothalamic functional connectivity. Headache, 64(1), 55–67. doi:10.1111/head.14656
- ↩ Leighton J, Lau C, Savdo A, Granata L (2025). Clinical treatment of cluster headache with the serotonergic indoleamine psychedelics psilocybin and LSD and with ketamine: A case series. Cephalalgia Reports. doi:10.1177/25158163251345472
- ↩ Post M (2014). Treatment of cluster headache symptoms using synthetic tryptamine N,N-diallyl-5-methoxytryptamine. Self-published.
- ↩ Post M (2015). Cluster headache patient survey: 5-MeO-DALT. Self-published.
- ↩ Dias BdF, Robinson CL, Villar-Martinez MD, Ashina S, Goadsby PJ (2025). Current and novel therapies for cluster headache: a narrative review. Pain and Therapy, 14, 1–19.
¿Te ha resultado útil esta página?
Capítulos
- 1. How psilocybin, LSD, and 5-MeO-DALT workWhat psilocybin, LSD, and 5-MeO-DALT are, why they help with cluster headaches, and what a small preventive dose feels like.
- 2. Preparing your doseHow to obtain, measure, and prepare a dose of psilocybin mushrooms, LSD, or 5-MeO-DALT to prevent cluster headaches.
- 3. The prevention protocolStep-by-step instructions for using small, spaced doses of psilocybin, LSD, or 5-MeO-DALT to prevent cluster headaches.
- 4. Safety and drug interactionsWhich medications are dangerous to combine with psilocybin, LSD, or 5-MeO-DALT, who should avoid them, and how to minimize risks.
- 5. LegalityWhere psilocybin, LSD, and 5-MeO-DALT are legal, decriminalized, or controlled, by country and US state.
- 6. Frequently asked questionsCommon questions and answers about using psilocybin, LSD, and 5-MeO-DALT to prevent cluster headaches.
Descargo de Responsabilidad
La información en este sitio web se proporciona únicamente con fines educativos y de reducción de daños. No constituye asesoramiento médico y no debe reemplazar la consulta con un profesional de salud calificado. Consulte nuestra página de Aviso Legal para más detalles.