How to take verapamil
How to dose verapamil for cluster headaches: starting dose, titration schedule, immediate-release vs extended-release, and timing suggestions.
Written by Alfredo Parra, PhD
This page covers what a typical verapamil regimen looks like. We focus on dose, timing, formulation, and how the protocol may differ between episodic and chronic patients.
The main takeaway from this chapter is that the most common reason verapamil fails is that the daily dose was never raised high enough to prevent attacks. A starting prescription of 40 to 240 mg/day is often what a primary-care physician will suggest, especially if they've used verapamil for high blood pressure but not for cluster headache. However, that is the bottom of the dose range, not the target. We will explain how to make sure your doctor increases your dose to a level that actually works, while minimizing risks.[1][2]
Starting dose and titration
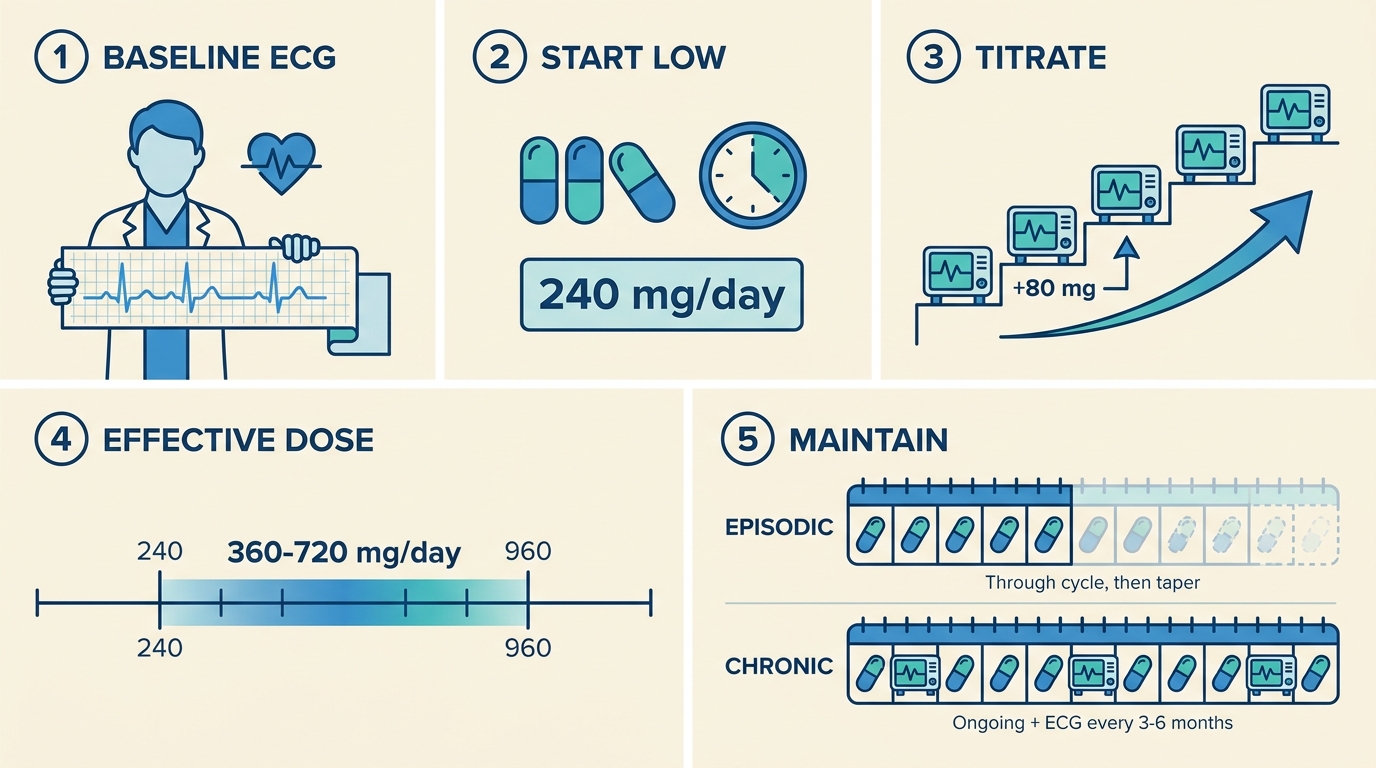
You will not start with a high dose. Verapamil is increased gradually, with electrocardiogram (ECG) checks before each increase.
There are two commonly used protocols.
The slower UK-style protocol:[3]
- Get a baseline ECG before the first dose.
- Start at 240 mg/day, taking 80 mg of immediate-release verapamil three times daily.
- Increase by 80 mg every 10 to 14 days (doing an ECG before increasing).
- Continue until your attacks are suppressed, side effects intervene, or you reach about 960 mg/day.
The faster European protocol:[4]
- Get a baseline ECG before the first dose.
- Start at 80 mg of immediate-release verapamil three or four times daily (240 to 320 mg/day).
- Increase by 80 mg every 3 to 4 days (faster than the UK-style protocol).
- Do an ECG before every 160 mg increment once you reach 480 mg/day.
- Stop at a maximum of around 1,000 mg/day, with cardiologist supervision at high doses.
Why two protocols? A slow titration can take longer than the duration of the cluster cycle itself. An episodic patient whose cycle lasts 6 to 8 weeks may end the bout before a +80 mg every 10 to 14 days schedule reaches a high-enough dose. European specialists tend to raise the dose faster, with closer ECG monitoring, while the cycle is still going. A retrospective comparison of +120 mg every 2 weeks versus +80 mg every 2 weeks in 169 patients found similar efficacy and side effects in both groups, suggesting that faster titration is safe when paired with proper monitoring.[5] Some specialists use this +120 mg every 2 weeks schedule as a practical compromise. It reaches the typical effective range (360 mg/day) within two weeks and the top of that range (720 mg/day) within eight. The diagrams below show what such a protocol could look like.
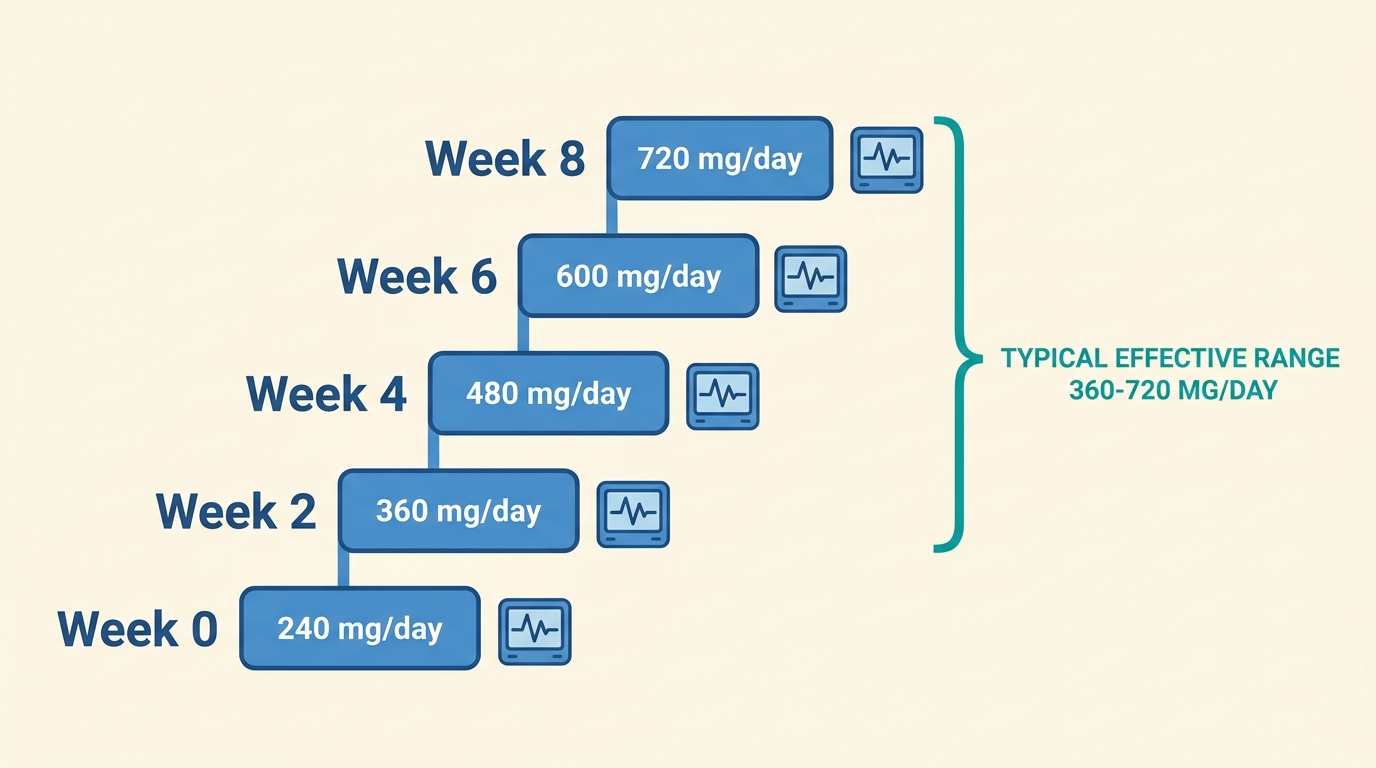 Example titration schedule: +120 mg every 2 weeks, reaching the effective range by week 2 and the upper end by week 8. Your doctor may recommend a slightly different protocol depending on your needs.
Example titration schedule: +120 mg every 2 weeks, reaching the effective range by week 2 and the upper end by week 8. Your doctor may recommend a slightly different protocol depending on your needs.
The target dose for most patients is 360 to 720 mg/day.[1][6] Chronic patients tend to need more than episodic patients. On average, chronic patients need around 572 mg/day versus 354 mg/day for episodic patients. Some patients respond at lower doses; some need 960 to 1,200 mg/day under specialist care.[7] Doses above 480 mg/day should trigger more frequent ECG monitoring and, in some health systems, a documented informed-consent conversation about off-label cardiac risk.[8]
Immediate-release versus extended-release
If you've been prescribed verapamil for cluster headache, ask whether it's immediate-release (IR) or extended/sustained-release (ER or SR). Headache specialists strongly prefer immediate-release for several reasons:
- Cluster attacks often come at predictable times. Immediate-release verapamil lets you take 3 to 4 doses spread across the day, with a larger dose timed to your attack window. Extended-release spreads the dose evenly across the day and can't be weighted that way.[6]
- All the positive cluster headache trial data (the Leone 2000 placebo-controlled trial and the Bussone 1990 verapamil-versus-lithium trial) used immediate-release.[9] Extended-release has never been formally tested in cluster headache.
- Titration is safer with immediate-release because the dose can be adjusted in 40 mg increments. Extended-release pills come in larger steps.
If your prescription is for extended-release, ask your doctor whether you can switch to immediate-release. Many primary-care doctors default to extended-release because that's the standard for blood pressure; few are aware of the specifics for cluster headache.
Daily timing and missed doses
How you spread your doses through the day matters as much as the total amount.
For most patients on immediate-release verapamil, the standard split is three to four times a day, roughly every 6 to 8 hours. If your attacks are nocturnal, it is recommended to take a larger dose in the evening and at bedtime. A common community practice for nocturnal attacks is:
- A smaller dose in the morning (e.g., 80 mg).
- A middle dose at midday (e.g., 80 mg).
- A larger dose in the evening (e.g., 160 mg).
- An optional bedtime dose (e.g., 80 mg), or a dose set on an alarm for 2 hours before your usual attack time.
For patients with predominantly morning attacks, some set an alarm and take a dose 2 hours before they usually wake. This is uncomfortable but reduces the attacks that still occur despite treatment.
If you miss a dose, do not just wait for the next scheduled one. Many patients report that a single missed dose triggers 2 to 5 days of attacks that still occur despite treatment. One commonly-shared workaround is that if you forget a dose, take the missed dose between the next two scheduled doses instead of skipping it. Set phone alarms if needed. Missing doses is a common cause of unexpected flare-ups.
Episodic versus chronic
The shape of a verapamil regimen depends on whether you have episodic or chronic cluster headache.
Episodic cluster headache
Begin verapamil as soon as a new cycle starts, or earlier if you can recognize the warning signs of a cycle beginning. Titrate up as fast as your protocol allows, ideally with a bridge treatment (typically prednisone or an occipital nerve block) to cover the first 2 to 3 weeks while the verapamil dose is increased.
During the cycle, stay on the effective dose throughout the bout, plus a few weeks past your last attack. Stopping too early may cause the attacks to come back.
When you've been attack-free for a few weeks and feel confident the cycle is over, taper down gradually. The standard practice is to mirror your titration in reverse (for example, reducing by 80 mg every 1 to 2 weeks).[4][8] Do not stop abruptly. Some patients report that stopping suddenly triggers rebound attacks, so if you've had a good response, treat the taper carefully.
Chronic cluster headache
If you have chronic cluster headache, verapamil is taken continuously and indefinitely.
Chronic patients usually need higher doses than episodic patients. Published mean effective doses are around 572 mg/day for chronic versus 354 mg/day for episodic.[6] Some patients take 720 to 960 mg/day long-term, and a minority need 1,200 mg/day under specialist care.
Efficacy is lower than in episodic patients, even at adequate doses. If verapamil only partly helps you, combining preventives (typically lithium, sometimes a CGRP-targeting drug) may be an option.
ECG monitoring is required indefinitely, not just during titration. Cardiac side effects can appear years after you've been stable on a dose.[7]
Summary of verapamil for episodic versus chronic patients
| Episodic | Chronic | |
|---|---|---|
| Duration of treatment | Cycle length plus 2 to 4 week taper | Indefinite |
| Typical effective dose | 240–480 mg/day (~354 mg mean) | 480–960 mg/day (~572 mg mean), sometimes 1,200 mg |
| Response rate (open-label, adequate dose) | ~94% complete relief | ~55% complete relief |
| Bridge treatment | Almost always needed (prednisone or occipital nerve block) | At a frequency determined by your doctor |
| Tapering | Mandatory; gradual | Not while on therapy; gradual if discontinuing |
| ECG cadence | Baseline plus before each escalation; can stop once tapered | Baseline plus before each escalation plus every 3–6 months indefinitely |
Combining verapamil with abortive treatments
Verapamil is a preventive. It does not stop attacks in progress. You'll still need an abortive treatment for the attacks that still occur despite treatment. Verapamil is routinely combined with high-flow oxygen, sumatriptan (injection or nasal spray), and, where legal and accessible, DMT. None of these has a known dangerous interaction with verapamil. With DMT in particular, there's no added cardiovascular concern, since verapamil lowers heart rate and blood pressure rather than raising them.
Verapamil is considered a partial "blocker" of the psychedelic prevention protocol (psilocybin, LSD) used by the patient community for breaking cluster cycles. The community generally recommends tapering off verapamil first if you plan to try psychedelic prevention, though some patients have managed to do both at lower verapamil doses.[2] If this is something you're considering, see our psychedelics guide.
References
- ↩ Tfelt-Hansen P, Tfelt-Hansen J (2009). Verapamil for cluster headache. Clinical pharmacology and possible mode of action. Headache, 49(1), 117–125. doi:10.1111/j.1526-4610.2008.01298.x
- ↩ Wold B (2025). Pocket Guide to Cluster Headaches (Complete Handbook 1.5). Clusterbusters. Link
- ↩ Cohen AS, Matharu MS, Goadsby PJ (2007). Electrocardiographic abnormalities in patients with cluster headache on verapamil therapy. Neurology, 69(7), 668–675. Link
- ↩ May A, Evers S, Goadsby PJ, Leone M, Manzoni GC, Pascual J, et al. (2023). European Academy of Neurology guidelines on the treatment of cluster headache. European Journal of Neurology, 30(10), 2955–2979. doi:10.1111/ene.15956
- ↩ Cordero-Schmidt G, Wallasch TM, Kropp P (2013). Fast and slow titration of verapamil in cluster headache. Journal of Headache and Pain, 14(Suppl 1), P45. Link
- ↩ Blau JN, Engel HO (2004). Individualizing treatment with verapamil for cluster headache patients. Headache, 44(10), 1013–1018. Link
- ↩ Lantéri-Minet M, Silhol F, Piano V, Donnet A (2011). Cardiac safety in cluster headache patients using the very high dose of verapamil (≥720 mg/day). Journal of Headache and Pain, 12(2), 173–178. doi:10.1007/s10194-010-0289-x
- ↩ Schmerzklinik Kiel (2023). G-BA verapamil for cluster headache. Schmerzklinik Kiel. Link
- ↩ Petersen AS, Barloese MCJ, Snoer A, Soerensen AMS, Jensen RH (2019). Verapamil and cluster headache: still a mystery. A narrative review of efficacy, mechanisms and perspectives. Headache, 59(8), 1198–1211. doi:10.1111/head.13603
Did you find this page helpful?
Disclaimer
The information on this website is provided for educational and harm reduction purposes only. It does not constitute medical advice and should not replace consultation with a qualified healthcare professional. See our Legal page for more details.