Preventing cluster headache attacks with verapamil
A complete guide to verapamil for cluster headaches: getting the dose right, taking it safely, and managing side effects.
Written by Alfredo Parra, PhD
The standard first-line preventive (at a sufficiently high dose)
Verapamil is a heart medication that has been the first-line preventive for cluster headache for about forty years. If your neurologist or headache specialist is familiar with cluster headache, verapamil will almost certainly be the first treatment they offer, regardless of whether your cluster headaches are episodic or chronic.
In a placebo-controlled randomized trial, 80% of episodic patients on 360 mg/day saw a 50% reduction in attacks after 14 days of taking verapamil, compared with 0% on placebo.[1] The 2023 European Academy of Neurology guideline gives it a strong recommendation, and in 2025 the World Health Organization added verapamil to its Model List of Essential Medicines specifically for cluster headache.[2][3] Interestingly, verapamil is currently used off-label for cluster headache, which means that no regulator has formally approved it specifically for cluster headache.
The doses used for cluster headache (360 to 960 mg/day, sometimes higher) are roughly double the doses used for blood pressure, and they require electrocardiogram (ECG) monitoring to use safely. About 1 in 5 patients on adequate doses show some change on the ECG during titration.[4] Almost all of those changes are mild and managed by adjusting the dose, but they're the reason monitoring is a must.
How to take verapamil for cluster headache
Verapamil is taken daily, at a dose that increases slowly over weeks. It is used to prevent future attacks rather than to abort an attack in progress.
A typical protocol might look as follows, starting at the beginning of your cluster cycle (or, ideally, shortly before; or anytime for chronic patients):
- Your doctor will do a baseline ECG. If everything looks good, you will then start taking 240 mg/day of immediate-release verapamil (80 mg three times daily).
- If you're in a cycle, a short course of prednisone (or an occipital nerve block) may be prescribed alongside verapamil. These treatments may reduce attacks during the 2 to 3 weeks while verapamil starts to take effect (but they cannot be used long-term).
- You then increase by 80 mg every 1 to 2 weeks, with an ECG before each increase. If you are already in your cycle, a faster increase might be possible.
- Most patients settle in the 360 to 720 mg/day range. However, some patients need 960 to 1,200 mg/day.
- Once you reach a working dose, you stay there. Episodic patients stay on verapamil through the whole cycle plus a few weeks, then taper down gradually. Chronic patients stay on it indefinitely.
- ECGs continue periodically for as long as you're on verapamil, usually every 3 to 6 months at high doses.
See the protocol page for the full regimen.
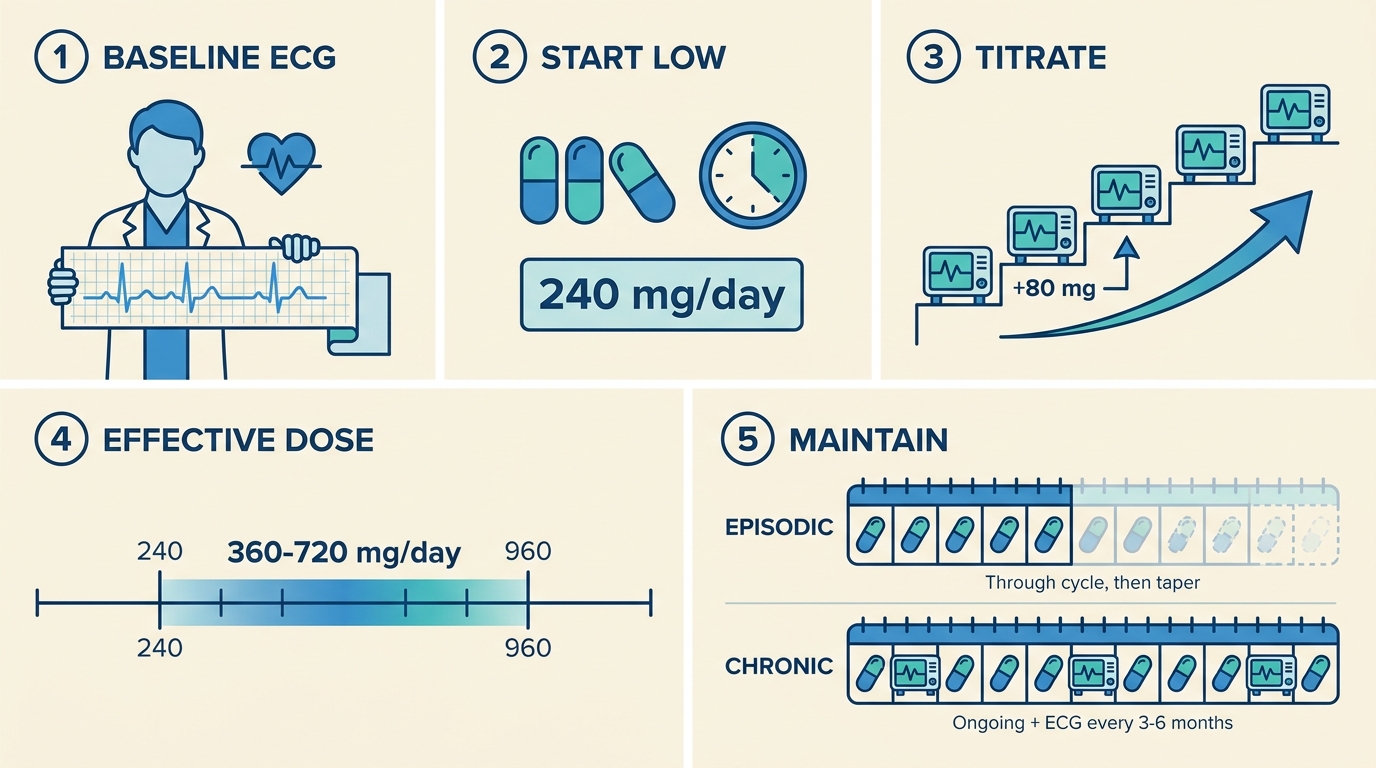 A typical verapamil protocol.
A typical verapamil protocol.
Verapamil's effectiveness
We don't have a very clear picture of what fraction of patients find relief, and to what extent, but the data we have is encouraging.
In an RCT, 80% of episodic patients saw a 50% reduction in attacks after 14 days of taking verapamil (on 360 mg/day).[1] In an open-label study, 94% of episodic patients and 55% of chronic patients reached complete relief.[5]
Data from patient surveys is more mixed. A meta-analysis of surveys by Rusanen and colleagues showed that only about 50% of patients who had tried verapamil responded positively.[6] However, it is likely that a large fraction of surveyed patients didn't follow the correct protocol (in particular, not reaching a high enough dose, or not waiting long enough).
For the meaningful minority who don't respond at any dose, other options exist. We recommend our guide on preventive treatments to learn more about them and find something that works for you.
References
- ↩ Leone M, D'Amico D, Frediani F, et al. (2000). Verapamil in the prophylaxis of episodic cluster headache: a double-blind study versus placebo. Neurology, 54(6), 1382–1385. Link
- ↩ May A, Evers S, Goadsby PJ, Leone M, Manzoni GC, Pascual J, et al. (2023). European Academy of Neurology guidelines on the treatment of cluster headache. European Journal of Neurology, 30(10), 2955–2979. doi:10.1111/ene.15956
- ↩ Tassorelli C, Lampl C, García-Azorín D, et al. (2026). WHO Model List of Essential Medicines additions for cluster headache. Cephalalgia. Link
- ↩ Cohen AS, Matharu MS, Goadsby PJ (2007). Electrocardiographic abnormalities in patients with cluster headache on verapamil therapy. Neurology, 69(7), 668–675. Link
- ↩ Blau JN, Engel HO (2004). Individualizing treatment with verapamil for cluster headache patients. Headache, 44(10), 1013–1018. Link
- ↩ Rusanen SS, De S, Schindler EAD, Artto VA, Storvik M (2022). Self-reported efficacy of treatments in cluster headache: a systematic review of survey studies. Current Pain and Headache Reports, 26(8), 623–637. Link
Did you find this page helpful?
Chapters
- 1. Verapamil basicsHow verapamil works for cluster headaches, the correct dose, who should not take it, and the most common side effects.
- 2. How to take verapamilHow to dose verapamil for cluster headaches: starting dose, titration schedule, immediate-release vs extended-release, and timing suggestions.
- 3. Safety and drug interactionsVerapamil drug interactions to avoid, who should not take it, what to check before starting, and what to do in an emergency.
- 4. Frequently asked questionsCommon questions about verapamil for cluster headache: dose, side effects, ECG monitoring, pregnancy, psychedelics, and how to talk to your doctor.
Disclaimer
The information on this website is provided for educational and harm reduction purposes only. It does not constitute medical advice and should not replace consultation with a qualified healthcare professional. See our Legal page for more details.