Diese Seite ist eine KI-generierte Übersetzung des Leitfadens aus dem Englischen. Wenn Sie Deutsch-Muttersprachler sind, helfen Sie uns bitte, diese Übersetzung zu verbessern, indem Sie die Schaltfläche „Diesen Leitfaden verbessern" am Ende der Seite verwenden.
Sicherheit und Arzneimittelwechselwirkungen
Welche Medikamente in Kombination mit Psilocybin, LSD oder 5-MeO-DALT gefährlich sind, wer sie meiden sollte und wie Sie Risiken minimieren.
Diese Substanzen sind in den zur Cluster-Kopfschmerz-Prophylaxe verwendeten Dosen körperlich sehr sicher. Anders als viele Cluster-Medikamente haben sie keine bekannte langfristige Organtoxizität, kein Suchtpotenzial und keine Entzugserscheinungen. Die wesentlichen Risiken entstehen durch Wechselwirkungen mit anderen Medikamenten, durch eine kleine Zahl von Vorerkrankungen und durch psychische Effekte bei zu hoher Dosierung. Diese Seite behandelt all dies im Detail. Bitte lesen Sie sie sorgfältig durch, bevor Sie Ihre erste Dosis nehmen.
Sicherheits-Checkliste
Arbeiten Sie jeden Punkt dieser Liste ab, bevor Sie Ihre erste Dosis nehmen.
- Medikamente aufgelistet. Ich habe alle Medikamente, Nahrungsergänzungsmittel und pflanzlichen Mittel notiert, die ich einnehme.
- Wechselwirkungen geprüft. Ich habe jedes davon mit der untenstehenden Medikamententabelle abgeglichen.
- Ärztliche Rücksprache (falls nötig). Wenn dies für meine Medikamente empfohlen wird (siehe Tabelle), habe ich mit meiner Ärztin oder meinem Arzt gesprochen.
- Serotonin-Syndrom verstanden. Ich kenne die Symptome und weiß, wann ich Hilfe rufen muss.
- Begleitperson organisiert. Ich habe eine vertrauenswürdige Person, die meinen Dosierungsplan kennt, insbesondere für meine erste Dosis.
- Triptan-Auswaschphase (falls zutreffend). Wenn ich Triptane einnehme, warte ich nach meiner letzten Dosis mindestens fünf Tage, bevor ich mit dem Protokoll beginne.
Arzneimittelwechselwirkungen im Überblick
Psilocybin, LSD und 5-MeO-DALT wirken alle auf das Serotoninsystem des Gehirns. Serotonin ist ein chemischer Botenstoff, mit dem Ihr Gehirn Stimmung, Schlaf und Schmerz reguliert. Viele gängige Medikamente greifen ebenfalls in dieses System ein. Wenn zwei oder mehr Wirkstoffe gleichzeitig auf Serotonin wirken, können sich ihre Effekte auf unerwünschte Weise summieren: Sie können nämlich einen Zustand auslösen, der als Serotonin-Syndrom bezeichnet wird.
Hier die Kurzfassung:
- Lithium ist ein striktes Ausschlusskriterium: Kombinieren Sie diese Substanzen nicht mit Lithium (Krampfanfall-Risiko).
- Serotonerge Medikamente und Substanzen (Wirkstoffe, die auf das Serotoninsystem zielen) erfordern ein Gespräch mit Ihrer Ärztin oder Ihrem Arzt. Die zwei Hauptkategorien sind:
- MAO-Hemmer. Mittleres bis hohes Risiko für ein Serotonin-Syndrom. Sie verhindern, dass Ihr Körper Tryptamine abbaut, und verstärken und verlängern die Wirkung dramatisch.
- SSRIs und SNRIs. Mittleres bis niedriges Risiko für ein Serotonin-Syndrom. Sie blockieren zudem in der Regel die Wirkung des Protokolls und müssen vor Beginn über einen längeren Zeitraum ausgeschlichen werden.
- Triptane, Ergotamine und viele Cluster-Prophylaktika (Verapamil, Prednison, Topiramat usw.) müssen mindestens fünf Tage vor Ihrer ersten Dosis abgesetzt werden. Sie blockieren die Wirkung des Protokolls.
- Alles andere: Sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt.
Überprüfen Sie Ihre Medikamente
Bevor Sie mit dem Protokoll beginnen, erstellen Sie eine Liste aller Mittel, die Sie einnehmen (Rezeptpflichtiges, rezeptfreie Medikamente, Nahrungsergänzungsmittel, pflanzliche Mittel) und gleichen Sie diese mit dieser Tabelle ab.
| Kategorie | Bezeichnungen / Beispiele | Risiko | Was zu tun ist |
|---|---|---|---|
| Lithium | Lithobid, Eskalith | Krampfanfall-Risiko: nicht kombinieren | Keine Alternative. Das Protokoll ist unter Lithium keine Option. Sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt über ein sicheres Ausschleichen, wenn Sie es versuchen möchten. |
| MAO-Hemmer | Phenelzin (Nardil), Tranylcypromin (Parnate), Isocarboxazid (Marplan), Moclobemid (Manerix); Antibiotikum: Linezolid; pflanzlich: Ayahuasca-Zubereitungen, Syrische Steppenraute, Changa. | Mittel-hoch: Serotonin-Syndrom-Risiko + verstärkte Wirkung | Sprechen Sie unbedingt mit Ihrer Ärztin oder Ihrem Arzt. Sorgen Sie immer für eine Begleitperson. Lesen Sie den Abschnitt zum Serotonin-Syndrom weiter unten. |
| SSRIs / SNRIs | Fluoxetin (Prozac), Sertralin (Zoloft), Paroxetin (Paxil), Citalopram (Celexa), Escitalopram (Lexapro), Venlafaxin (Effexor), Duloxetin (Cymbalta), Desvenlafaxin (Pristiq). | Mittel-niedrig: Serotonin-Effekte können sich aufsummieren; blockiert zudem das Protokoll | Sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt. SSRIs müssen vor Beginn häufig über Wochen langsam ausgeschlichen werden. Setzen Sie Antidepressiva niemals ohne ärztliche Aufsicht ab. |
| Triptane | Sumatriptan (Imitrex), Rizatriptan (Maxalt), Zolmitriptan (Zomig), Naratriptan (Amerge), Frovatriptan (Frova), Almotriptan (Axert), Eletriptan (Relpax). | Geringes Serotonin-Risiko; das Hauptproblem ist, dass sie die Wirkung des Protokolls blockieren. | Warten Sie nach Ihrer letzten Triptan-Dosis mindestens fünf Tage, bevor Sie mit dem Protokoll beginnen. Vermeiden Sie eine Wiederaufnahme während des Protokolls. |
| Ergotamine | Dihydroergotamin (DHE), Methysergid (Sansert), Cafergot, Ergotamintartrat (Ergomar). | Blockieren die Wirkung des Protokolls. | Mindestens fünf Tage vor Ihrer ersten Dosis absetzen. |
| Cluster-Prophylaktika | Verapamil (Isoptin, Verelan, Calan), Kortikosteroide (Prednison, Prednisolon, Dexamethason), Topiramat (Topamax), Natriumvalproat (Depakote), Carbamazepin (Tegretol). | Blockieren die Wirkung des Protokolls. | Sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt über ein sicheres Absetzen. Einige müssen ausgeschlichen werden. Warten Sie nach dem Absetzen mindestens fünf Tage, bevor Sie Ihre erste Dosis nehmen. |
| Andere serotonerge Substanzen | Trizyklische Antidepressiva (Amitriptylin, Nortriptylin, Imipramin, Clomipramin), Opioide (Tramadol, Methadon, Fentanyl, Hydrocodon, Oxycodon), Dextromethorphan (in vielen Hustenmitteln), Johanniskraut, Amphetamine (Adderall, Vyvanse), MDMA / Ecstasy. | Variabel: hängt von der Kombination ab | Sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt. Mehrere serotonerge Substanzen gemeinsam können sich zu einem erheblichen Risiko aufsummieren, auch wenn jede für sich genommen sicher erscheint. |
| Alkohol & Nikotin | Bier, Wein, Spirituosen; Zigaretten, Zigarren, Kautabak, Schnupftabak. | Niedrig (nicht serotonerg); beides sind jedoch bekannte Cluster-Kopfschmerz-Trigger. | An Dosistagen und am Tag danach meiden. Viele Cluster-Patienten verzichten während eines Zyklus ganz darauf. |
Wenn Ihr Medikament nicht auf dieser Liste steht, gehen Sie nicht davon aus, dass es sicher ist. Suchen Sie online nach dem Namen Ihres Medikaments plus „Serotonin" oder fragen Sie Ihre Ärztin, Ihren Arzt oder Ihre Apotheke.
So sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt
Viele Ärztinnen und Ärzte kennen sich nur begrenzt mit psychedelika-gestützten Behandlungen aus, und Sie befürchten möglicherweise, verurteilt zu werden. Hier ein Vorschlag, wie Sie vorgehen können:
-
Stellen Sie es als Schadensminimierung dar. „Ich habe Cluster-Kopfschmerzen und habe gelesen, dass Menschen kleine Dosen Psilocybin (oder LSD oder 5-MeO-DALT) zur Vorbeugung von Attacken einsetzen. Ich möchte sicherstellen, dass das mit meinen Medikamenten sicher ist, und hätte dabei gerne Ihre Unterstützung."
-
Bringen Sie diese Seite mit. Zeigen Sie die obige Medikamententabelle und den Abschnitt zum Serotonin-Syndrom weiter unten. Ärztinnen und Ärzte reagieren gut auf konkrete, präzise Fragen.
-
Fragen Sie nach Ihren konkreten Medikamenten. „Könnten Sie prüfen, ob eines meiner Medikamente mit einem Serotonin-Rezeptor-Agonisten wechselwirkt?"
-
Wissen Sie, dass man Sie nicht melden kann. Arzt-Patienten-Gespräche unterliegen der Schweigepflicht. Ihre Ärztin oder Ihr Arzt darf abraten, kann Sie aber nicht bei den Strafverfolgungsbehörden anzeigen, nur weil Sie fragen.
-
Wenn sich Ihre Ärztin oder Ihr Arzt weigert, sich mit dem Thema zu befassen, ist das ein Signal, sich nach Möglichkeit eine zweite Meinung einzuholen. Manche Neurologinnen und Neurologen, Kopfschmerzspezialistinnen und -spezialisten sowie Psychiaterinnen und Psychiater kennen die Patientenpraxis und können zur sicheren Anwendung beraten.
Serotonin-Syndrom: Was Sie wissen müssen
Ein Serotonin-Syndrom entsteht, wenn Ihr Gehirn mit zu viel Serotonin überflutet wird. Es tritt am ehesten auf, wenn eine dieser Substanzen mit einem anderen Wirkstoff kombiniert wird, der ebenfalls den Serotoninspiegel anhebt — insbesondere mit MAO-Hemmern oder mit mehreren sich aufsummierenden serotonergen Substanzen. Es ist behandelbar, und das Kennen der Anzeichen ist es, was es beherrschbar statt gefährlich macht.
Das Risiko steigt mit höheren Dosen und mehr serotonergen Substanzen, aber es ist schwer vorherzusagen, welche Kombination oder Dosis es genau auslösen wird. Deshalb empfehlen wir, mit Ihrer Ärztin oder Ihrem Arzt zu sprechen, mit niedrigen Dosen zu beginnen und eine Begleitperson dabei zu haben.
Symptome
Rufen Sie sofort den Rettungsdienst, wenn eines dieser schweren Symptome auftritt:
- Krampfanfall (unkontrolliertes Zittern, Bewusstseinsverlust).
- Hohes Fieber (über 38,5 °C / 101,3 °F).
- Ohnmacht.
- Starke Muskelkrämpfe oder Muskelsteifigkeit (Ihr Körper fühlt sich verkrampft an).
- Unkontrollierbare seitliche Augenbewegungen.
- Schneller oder unregelmäßiger Herzschlag in Verbindung mit starkem Unwohlsein.
- Jegliches Symptom (auch die leichteren weiter unten), das sich rasch verschlimmert.
Rufen Sie Ihre Ärztin oder Ihren Arzt an, wenn diese leichteren Symptome auftreten:
- Schneller Herzschlag, Schüttelfrost oder starkes Schwitzen, das länger als 30 Minuten anhält.
- Muskelzucken oder -rucken.
- Übelkeit oder Durchfall.
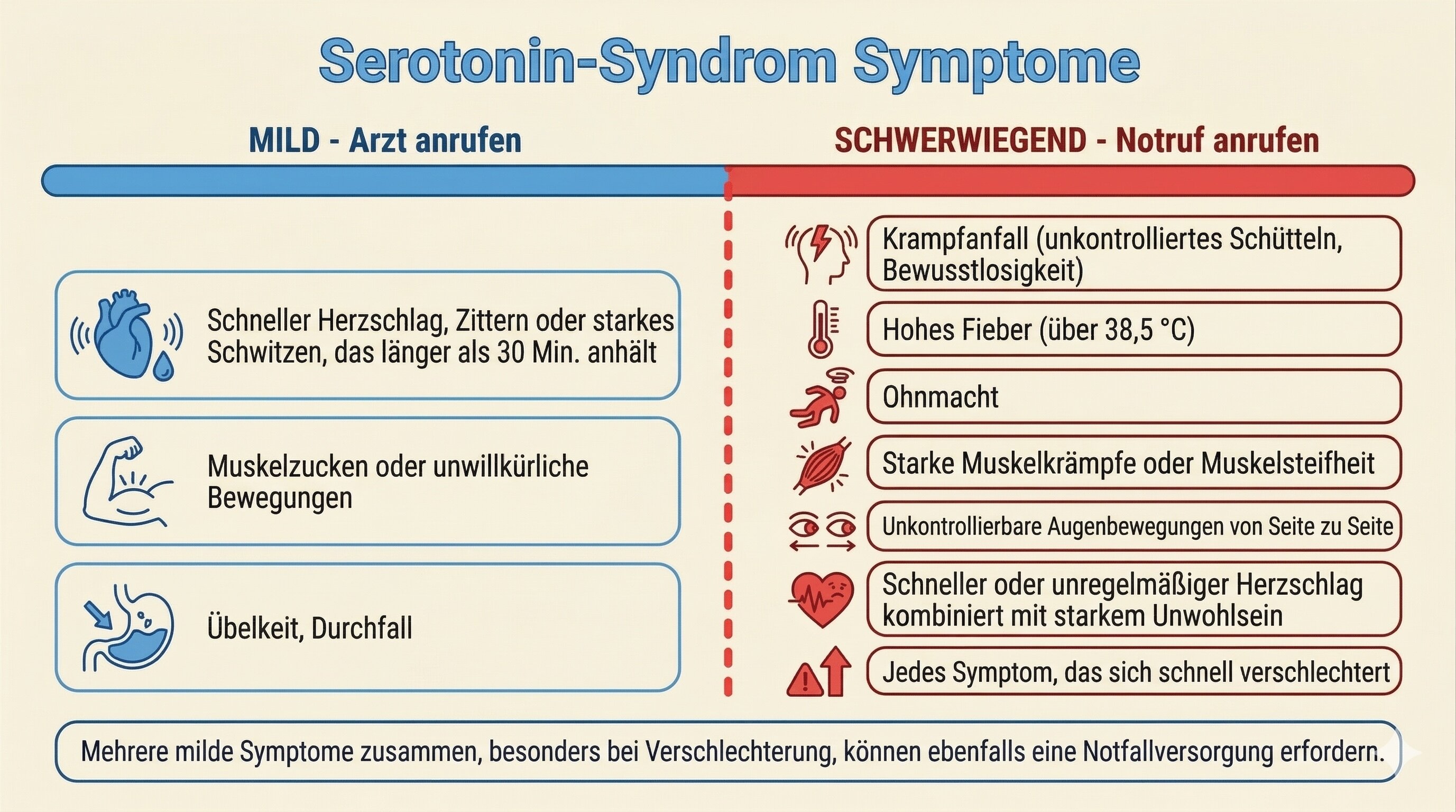
Die Symptome eines Serotonin-Syndroms reichen von leicht (links) bis schwer (rechts). Die rote Linie markiert, wann der Rettungsdienst zu rufen ist.
Falls Sie jemals notärztliche Hilfe brauchen, ist es entscheidend, dass das medizinische Team weiß, was Sie eingenommen haben. Sagen Sie ihnen, dass Sie Psilocybin (oder LSD oder 5-MeO-DALT) eingenommen haben, und nennen Sie alle weiteren Medikamente. Ein Serotonin-Syndrom ist behandelbar, muss aber richtig erkannt werden.
Weiterführende Quellen
- Demystifying Serotonin Syndrome (Canadian Family Physician) — enthält ein druckbares Patienteninformationsblatt.
- Serotonin Syndrome (Cleveland Clinic).
- Serotonin Syndrome (Mayo Clinic).
Arzneimittelwechselwirkungen im Detail
Dieser Abschnitt erläutert jede Medikamentenkategorie aus der obigen Tabelle ausführlicher. Lesen Sie die Teile, die auf Sie zutreffen.
Lithium
Lithium ist ein Stimmungsstabilisator, der bei bipolarer Störung verschrieben wird und auch zur Vorbeugung von Cluster-Kopfschmerzen eingesetzt wird. Die Kombination von Lithium mit Psilocybin oder LSD kann Krampfanfälle auslösen. Den direktesten Hinweis liefert eine Johns-Hopkins-Analyse von Online-Erfahrungsberichten aus dem Jahr 2021: Von 62 Berichten, die die Kombination eines klassischen Psychedelikums mit Lithium beschrieben, gingen 47 % mit Krampfanfällen einher und 39 % mit einer ärztlichen Vorstellung. Im Gegensatz dazu kam es bei 0 von 34 Berichten zu Psychedelika in Kombination mit Lamotrigin (einem anderen Stimmungsstabilisator) zu Krampfanfällen.[2] Der Mechanismus ist nicht vollständig verstanden, und es gibt keine spezifischen Daten zu 5-MeO-DALT, aber die vorsichtige Annahme ist, dass das gleiche Risiko gilt.
Wenn Sie Lithium einnehmen, beginnen Sie nicht mit diesem Protokoll. Sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt über ein sicheres Ausschleichen, wenn Sie es versuchen möchten. Lithium hat eine enge therapeutische Breite und muss unter ärztlicher Aufsicht langsam ausgeschlichen werden.
MAO-Hemmer
MAO-Hemmer (Monoaminoxidase-Hemmer) sind Medikamente, die die Fähigkeit des Körpers verlangsamen, Serotonin und Tryptamine abzubauen. Daraus ergeben sich in Kombination mit Psilocybin oder 5-MeO-DALT zwei separate Bedenken (LSD wird über einen anderen Stoffwechselweg abgebaut und ist weniger betroffen, dennoch ist Vorsicht geboten):
- Serotonin-Syndrom. Da MAO-Hemmer verhindern, dass Ihr Körper Serotonin normal abbaut, kann sich Serotonin auf gefährliche Werte anhäufen. Symptome können während oder sogar Stunden nach der Einnahme der Dosis auftreten. Siehe Abschnitt zum Serotonin-Syndrom weiter oben.
- Verstärkte und verlängerte Wirkung. MAO-Hemmer machen oral wirksame Tryptamine dramatisch stärker und länger wirksam. Eine Dosis, die normalerweise milde prophylaktische Wirkungen entfalten würde, kann stattdessen eine intensive psychedelische Erfahrung hervorrufen.
Häufige MAO-Hemmer sind:
- Verschreibungspflichtige Antidepressiva: Phenelzin (Nardil), Tranylcypromin (Parnate), Isocarboxazid (Marplan), Moclobemid (Manerix).
- Antibiotika: Linezolid.
- Pflanzlich: Ayahuasca-Zubereitungen, Syrische Steppenraute (Harmal), Changa-Mischungen (die häufig Harmin oder Harmalin enthalten).
Wenn Sie einen MAO-Hemmer einnehmen, müssen Sie vor Beginn mit Ihrer Ärztin oder Ihrem Arzt sprechen. Wenn diese ihr Einverständnis gibt, sorgen Sie immer für eine Begleitperson, die die Symptome eines Serotonin-Syndroms kennt, und lassen Sie sie mindestens eine Stunde danach bei sich bleiben. Bei MAO-Hemmern können sich Symptome verzögert einstellen.
SSRIs und SNRIs
SSRIs und SNRIs sind sehr häufig verschriebene Antidepressiva. Sie wirken, indem sie den Serotoninspiegel im Gehirn erhöhen. In Kombination mit Psilocybin, LSD oder 5-MeO-DALT (die ebenfalls Serotonin-Rezeptoren aktivieren) gibt es zwei Probleme:
- Aufsummieren serotonerger Effekte. Das Risiko eines Serotonin-Syndroms durch eine kleine prophylaktische Dosis in Kombination mit einem einzelnen SSRI oder SNRI gilt allgemein als gering, ist aber nicht null — insbesondere, wenn Sie zusätzlich andere serotonerg wirkende Medikamente einnehmen.
- Blockade des Protokolls. SSRIs und SNRIs gehören außerdem zu den zuverlässigsten Blockern dieser Substanzen. Patienten unter SSRIs stellen häufig fest, dass das Protokoll schlicht nicht funktioniert, bis das SSRI aus dem Körper geklärt ist.
Häufige SSRIs: Citalopram (Celexa), Escitalopram (Lexapro), Fluoxetin (Prozac), Fluvoxamin (Luvox), Paroxetin (Paxil), Sertralin (Zoloft).
Häufige SNRIs: Venlafaxin (Effexor), Duloxetin (Cymbalta), Desvenlafaxin (Pristiq).
Sprechen Sie mit Ihrer Ärztin oder Ihrem Arzt, bevor Sie das Protokoll mit einem SSRI oder SNRI kombinieren. Sorgen Sie für eine Begleitperson bei Ihren ersten Dosen und stellen Sie sicher, dass diese die Symptome eines Serotonin-Syndroms kennt.
Triptane
Triptane (Sumatriptan usw.) werden häufig zur Beendigung von Cluster-Attacken eingesetzt. Es gibt zwei Bedenken:
- Blockade des Protokolls. Dies ist im Hinblick auf die Prophylaxe das größere Problem. Triptane gehören zu den zuverlässigsten Blockern. Patienten, die während des Protokolls weiter Triptane verwenden, stellen typischerweise fest, dass es nicht wirkt.
- Serotonin-Syndrom. Triptane interagieren mit dem Serotoninsystem, aber die aktuelle Evidenz legt nahe, dass sie kaum nennenswert zu einem Serotonin-Syndrom beitragen. Dennoch ist Vorsicht geboten, insbesondere wenn Sie weitere serotonerge Medikamente einnehmen.
Empfehlung: Warten Sie nach Ihrer letzten Triptan-Dosis mindestens fünf Tage, bevor Sie mit dem Protokoll beginnen. Ausnahme: Frovatriptan (Frova) hat eine längere Halbwertszeit, warten Sie hier mindestens sieben Tage. Viele Patienten stellen fest, dass sie Triptane deutlich seltener brauchen, sobald das Protokoll wirkt.
Andere serotonerge Substanzen
Viele gängige Medikamente beeinflussen Serotonin, auch wenn das nicht ihr Hauptzweck ist. Für sich genommen haben die meisten ein geringes Wechselwirkungsrisiko. Aber mehrere serotonerge Substanzen gemeinsam können sich zu einem erheblichen Risiko aufsummieren, auch wenn jede für sich genommen sicher erscheint.
Zu dieser Kategorie zählen:
- Trizyklische Antidepressiva (TCAs): Clomipramin, Imipramin, Amitriptylin, Nortriptylin.
- Opioide Schmerzmittel: Tramadol, Methadon, Meperidin, Fentanyl. Hinweis: Morphin hat keine gefährliche Serotonin-Wechselwirkung.
- Hustenstiller: Dextromethorphan (DXM), enthalten in vielen rezeptfreien Erkältungs- und Hustenmitteln.
- Pflanzlich: Johanniskraut, ein häufiges pflanzliches Nahrungsergänzungsmittel zur Stimmungsaufhellung.
- Stimulanzien: Amphetamin (Adderall, Vyvanse).
- Freizeitdrogen: MDMA / Ecstasy.
- Antihistaminika: Chlorpheniramin, Brompheniramin.
Alkohol und Nikotin
Alkohol und Tabak sind bekannte Auslöser für Cluster-Kopfschmerz-Attacken während eines Zyklus. Die meisten Patienten meiden sie ohnehin bereits. Darüber hinaus gibt es zwei spezifische Gründe, sie rund um die Einnahme zu meiden:
- Meiden Sie Alkohol an Dosistagen und am Tag danach. Er kann die Erfahrung unvorhersehbar verstärken und das Protokoll stören.
- Meiden Sie starken Tabakkonsum während der Dosis. Einige Patienten berichten, dass Übelkeit mit Nikotin stärker ausfällt.
Ein Wort zu Opiaten
Die Aufnahme von Opiaten in die Liste der Blocker stammt aus der Patientenliste der Clusterbusters-Community[1] und basiert auf gesammelten Erfahrungen, dass sie die Wirkung des Protokolls abschwächen können. Die pharmakologische Grundlage ist weniger gut belegt als bei den anderen oben genannten Kategorien, aber eine kleine Zahl älterer tierexperimenteller Studien hat gezeigt, dass Opioide und serotonerge Psychedelika auf Rezeptorebene interagieren können, wobei Opioide in niedrigen Dosen halluzinogene Effekte antagonisieren.[3] Patienten wird geraten, im Zweifel mehrere Tage vor der Einnahme — in Absprache mit der verschreibenden Ärztin oder dem verschreibenden Arzt — Opiate abzusetzen oder zu reduzieren.
Medikamente, die allgemein als sicher gelten
Die folgenden Mittel sind nicht dafür bekannt, in nennenswerter Weise mit diesen Substanzen zu interagieren:[1]
- Antibiotika (außer Linezolid, siehe MAO-Hemmer).
- NSAR (nichtsteroidale Antirheumatika): Aspirin, Acetaminophen / Paracetamol, Ibuprofen, Naproxen, Indometacin.
- Antazida und Magengeschwür-Medikamente.
- Asthma-Medikamente.
- Insulin.
- Koffein und Energydrinks.
- B-Komplex und Multivitamine.
- Die meisten Blutdruckmedikamente (z. B. Diovan), besprechen Sie dies jedoch mit Ihrer Ärztin oder Ihrem Arzt, wenn Sie kardiovaskuläre Bedenken haben.
- Statine (z. B. Lipitor).
- Mittel gegen Übelkeit (Meclizin, Dimenhydrinat).
Diese Liste ist nicht vollständig. Wenn Sie ein Medikament einnehmen, das hier nicht erwähnt ist, schlagen Sie es nach oder fragen Sie eine fachkundige Ärztin oder einen fachkundigen Arzt, bevor Sie weitermachen.
Wer diese Substanzen NICHT nehmen sollte
Schwangerschaft
Nehmen Sie kein Psilocybin, LSD oder 5-MeO-DALT, wenn Sie schwanger sind, schwanger werden möchten oder stillen. Tryptamin-Verbindungen können Gebärmutterkontraktionen auslösen und ein Risiko für den sich entwickelnden Fötus darstellen.
Persönliche oder familiäre Vorgeschichte von Psychosen
Bei diesen niedrigen Dosen können diese Substanzen in seltenen Fällen psychotische Episoden auslösen oder verschlimmern. Patienten, bei denen eine psychotische Störung diagnostiziert wurde — oder deren leibliche Eltern oder Geschwister davon betroffen sind — wird geraten, keine dieser Substanzen zu nehmen. Zu psychotischen Störungen zählen Schizophrenie, schizoaffektive Störung, wahnhafte Störung sowie schwere Formen einiger affektiver Störungen. Eine große Metaanalyse ergab, dass die Inzidenz einer psychedelika-induzierten Psychose in Bevölkerungsstudien bei etwa 0,002 % liegt.[4]
Persönliche oder familiäre Vorgeschichte einer bipolaren Störung
Die bipolare Störung ist ein Sonderfall. Die meisten modernen klinischen Psilocybin-Studien haben sowohl Personen mit bipolarer Störung als auch Personen mit erstgradigen Verwandten (Eltern, Geschwister, Kinder), die davon betroffen sind, ausgeschlossen. Die Sorge ist, dass Psychedelika bei genetisch prädisponierten Personen in seltenen Fällen eine manische oder psychotische Episode auslösen könnten. Ein 2024 erschienenes Review der verfügbaren Evidenz kam zu dem Schluss, dass das Risiko von Faktoren wie der Bipolar-Form in der Familie, dem Verwandtschaftsgrad und dem eigenen Alter abhängt, und schlug einen differenzierteren Ansatz als pauschalen Ausschluss vor.[5] Die ehrliche Zusammenfassung lautet: Das Risiko ist real, für die meisten Menschen in dieser Kategorie aber wahrscheinlich klein und schwer genau zu quantifizieren.
Wenn in Ihrer engsten Familie eine bipolare Störung vorkommt, besprechen Sie dies bitte mit einer Psychiaterin oder einem Psychiater, bevor Sie das Protokoll in Erwägung ziehen. Wenn Sie selbst eine bipolare Störung haben, ist das Risiko deutlich höher, und wir empfehlen, diese Substanzen nicht zu verwenden.
Herzerkrankungen, Bluthochdruck oder Schlaganfall in der Vorgeschichte
Tryptamine und Lysergamide verursachen während der Dosis einen kleinen, vorübergehenden Anstieg von Herzfrequenz und Blutdruck, vergleichbar mit leichter körperlicher Anstrengung. Für die meisten Menschen ist das harmlos. Wenn Sie eine schwere Herzerkrankung, unkontrollierten Bluthochdruck, einen Schlaganfall in der Vorgeschichte oder erhebliche Durchblutungsstörungen haben, sprechen Sie vor dem Weitermachen mit Ihrer Ärztin oder Ihrem Arzt.
Lebererkrankungen
Psilocybin, LSD und 5-MeO-DALT werden über die Leber verstoffwechselt. Wenn Sie eine erhebliche Lebererkrankung haben, sprechen Sie zunächst mit Ihrer Ärztin oder Ihrem Arzt.
Set und Setting
„Set und Setting" bezeichnet Ihren mentalen Zustand („Set") und Ihre physische Umgebung („Setting") zum Zeitpunkt der Einnahme. Beides kann den Verlauf der Erfahrung prägen. Selbst bei den hier verwendeten kleinen prophylaktischen Dosen, bei denen die psychoaktiven Effekte meist mild sind, sind Set und Setting wichtig.
- Dosieren Sie nicht in einer emotionalen Krise. Diese Substanzen während oder unmittelbar nach einem einschneidenden emotionalen Ereignis (einer Trennung, einem Todesfall, einem schweren Streit) einzunehmen, kann solche Gefühle in nicht hilfreicher Weise verstärken. Wenn etwas Schweres in Ihrem Leben passiert, verschieben Sie die Dosis nach Möglichkeit um ein paar Tage.
- Wählen Sie einen ruhigen, vertrauten Ort. Ihr Zuhause ist meist am besten. Gedämpftes Licht, ein bequemer Sessel oder ein Sofa, Wasser, Musik und ein Snack in Reichweite.
- Sorgen Sie dafür, dass eine nüchterne, vertrauenswürdige Person Ihren Dosierungsplan kennt. Besonders beim ersten Mal sollte jemand, dem Sie vertrauen, wissen, was Sie tun, und erreichbar sein.
- Fahren Sie nicht Auto, bedienen Sie keine Maschinen und treffen Sie keine wichtigen Entscheidungen während der Dosis. Dies gilt für die gesamte Wirkungsdauer, die bei LSD 8 Stunden oder mehr betragen kann.
Häufige Nebenwirkungen
Bei den kleinen Dosen, die zur Prophylaxe verwendet werden, sind die Nebenwirkungen meist mild und halten nur so lange an, wie die Dosis wirkt.
Psilocybin und LSD
- Leichte Übelkeit in der ersten Stunde.
- Leichte Körperwärme oder „Buzz".
- Stimmungsaufhellung oder Kicheranfälle.
- Leichte Geräusch- oder Lichtempfindlichkeit.
- Subtile visuelle oder sensorische Veränderungen.
- Leicht erhöhter Herzschlag.
- Verstärkte Emotionalität.
5-MeO-DALT
- Verringerte Körpertemperatur, kalte Finger und Zehen (die häufigste Nebenwirkung, bei 41 % der Befragten).[6]
- Leichter Schwindel oder Übelkeit (22 %).
- Deutliche Schläfrigkeit und starke Entspannung.
- 33 % der Befragten berichteten überhaupt keine Nebenwirkungen.
Nebenwirkungen einer höheren Dosis (z. B. 25 mg oder mehr DALT oder mehr als 1 g Pilze) sind tendenziell stärkere Ausprägungen derselben Effekte. Bleiben Sie bei den im Protokoll beschriebenen niedrigen Dosen, sofern Sie keinen konkreten Grund haben, sie zu erhöhen.
Wann Sie aufhören und ärztliche Hilfe suchen sollten
Suchen Sie ärztliche Hilfe, wenn Sie eines der folgenden Symptome erleben:
- Brustschmerzen, schwere Atemnot oder Schlaganfallzeichen (verwaschene Sprache, plötzliche einseitige Schwäche).
- Einen Krampfanfall.
- Schwere Verwirrtheit, die sich nicht legt, wenn die Dosis nachlässt.
- Ein klarer Realitätsverlust (Stimmenhören, ausgeprägter Wahn), der über die Wirkdauer der Dosis hinaus anhält.
- Symptome eines Serotonin-Syndroms, die schwer sind oder sich verschlimmern.
- Suizidgedanken, die sich Ihrer Kontrolle entziehen.
Cluster-Kopfschmerz selbst geht mit einer hohen Rate an Suizidgedanken einher und wird deshalb manchmal „Selbstmord-Kopfschmerz" genannt. Wenn Sie zu irgendeinem Zeitpunkt solche Gedanken haben, ob während des Protokolls oder nicht, wenden Sie sich bitte an eine Telefonseelsorge, eine vertraute Person oder Ihre Ärztin oder Ihren Arzt.
References
- ↩ Clusterbusters (2024). Alternative Treatments. Clusterbusters. Link
- ↩ Nayak SM, Gukasyan N, Barrett FS, Erowid E, Erowid F, Griffiths RR (2021). Classic psychedelic coadministration with lithium, but not lamotrigine, is associated with seizures: an analysis of online psychedelic experience reports. Pharmacopsychiatry, 54(5), 240–245. doi:10.1055/a-1524-2794
- ↩ Glennon RA (1986). Opioid-hallucinogen interactions. Pharmacology Biochemistry and Behavior, 24(6), 1655–1665. Link
- ↩ Sabé M, Sulstarova A, Glangetas A, De Pieri M, Mallet L, Curtis L, et al. (2025). Reconsidering evidence for psychedelic-induced psychosis: An overview of reviews, a systematic review, and meta-analysis of human studies. Molecular Psychiatry, 30(3), 1223–1255. doi:10.1038/s41380-024-02800-5
- ↩ Downey AE, Bradley ER, Lerche AS, O'Donovan A, Krystal AD, Woolley J (2024). A plea for nuance: should people with a family history of bipolar disorder be excluded from clinical trials of psilocybin therapy?. Psychedelic Medicine, 2(2), 61–70. doi:10.1089/psymed.2023.0051
- ↩ Post M (2015). Cluster headache patient survey: 5-MeO-DALT. Self-published.
War diese Seite hilfreich?
Haftungsausschluss
Die Informationen auf dieser Website dienen ausschließlich Bildungszwecken und der Schadensminimierung. Sie stellen keine medizinische Beratung dar und sollten nicht die Konsultation einer qualifizierten medizinischen Fachkraft ersetzen. Weitere Einzelheiten finden Sie auf unserer Seite Rechtliche Hinweise .