Aborting an attack with oxygen
How to use oxygen during a cluster attack. Done well, it ends the pain within minutes for most patients. When it doesn't, the culprit is usually equipment, flow, or breathing technique, all of which can be fixed.
Used well, oxygen ends a cluster attack within minutes for most patients. But it's not unusual to struggle with making oxygen work at first. When it seems to fail, the common culprits are incorrect equipment, flow, or breathing technique, and all of them can be addressed. This chapter walks through the abort procedure, the breathing techniques that work for most patients, and how to experiment to find what works best for you.
The abort procedure at a glance
This procedure works for any setup, demand valve or reservoir bag, mask or mouthpiece. Two parts of your kit are involved here: the cylinder valve (the knob on top of the tank that releases the gas) and the regulator (the device fitted below it, carrying the flow dial or demand valve). If these or other terms are unfamiliar, read the Equipment chapter first.
Speed matters. You want to go through the steps just below at the first sign that an attack might be coming.
- Turn on the oxygen: First make sure the regulator is turned off or set to its lowest flow. Then open the cylinder valve. Finally, set the regulator to the desired flow, or, if you're using a demand valve, simply turn on the regulator.
- Sit upright or stand. Then put on your mask or mouthpiece and start breathing using one of the patterns below.
- Keep going at the same pace until the pain is completely gone. Typical relief comes in 5–15 minutes. If oxygen still doesn't work after 15 minutes, consider a rescue medication (see just below).
- Stay on oxygen for at least 5 minutes after the pain is gone. When the pain is gone, lower the flow rate and breathe deeply but more slowly. Stopping the moment relief hits can trigger a bounce-back. See Staying on after the pain stops below.
- When you're done, turn off the regulator, then close the cylinder valve. Ventilate the room. Don't smoke or produce sparks until the room is well-aired.
- Note what you did and how it went. Once you've recovered, take a minute to jot down your setup, breathing technique, and how the attack responded. See Keeping notes below.
Things that can help alongside oxygen (see the remedies chapter):
- Caffeine (coffee, energy drink, or a caffeine pill) at the first sign. Use with caution if you have cardiovascular issues.
- Cold on the painful side. An ice pack against the temple, or a sip of ice water held briefly against the palate on the painful side.
If oxygen isn't aborting the attack after about 15 minutes, consider a rescue medication. Sumatriptan given as an injection under the skin (subcutaneous) typically acts within 10–15 minutes and is a first-line abortive; zolmitriptan given as a nasal spray (intranasal) is a slower alternative. Both are triptans, a class of prescription medication, so arrange them with your doctor in advance, before you need them. Vaped DMT, where you have access, is faster than either. You can keep breathing oxygen while the rescue medication takes effect. See the Treatment overview and the DMT guide. Use oxygen first when you can: it has no daily limit, while triptans are typically limited to two doses in 24 hours.
Breathing techniques
There isn't one universally best way to breathe during an oxygen abort. Two families of technique dominate patient practice. Hyperventilation pairs naturally with a demand valve and is widely considered the fastest way to abort an attack with oxygen. Deep breathing pairs naturally with a reservoir-bag setup (a ClusterO2 kit or non-rebreather mask), although hyperventilation can also be used with those setups if the oxygen flow is high enough. The best technique is ultimately the one that quickly ends the pain for you, so we encourage you to experiment with every technique your equipment allows.
Hyperventilation
The technique
Breathe as fast as you physically can: a full inhale, a full exhale, repeated with no pause.
Breathing hard can leave you light-headed, dizzy, or tingly in the hands and face. That is normal, harmless, and passes within a minute of slowing down. If you feel you might faint, slow your breathing but stay on the oxygen.
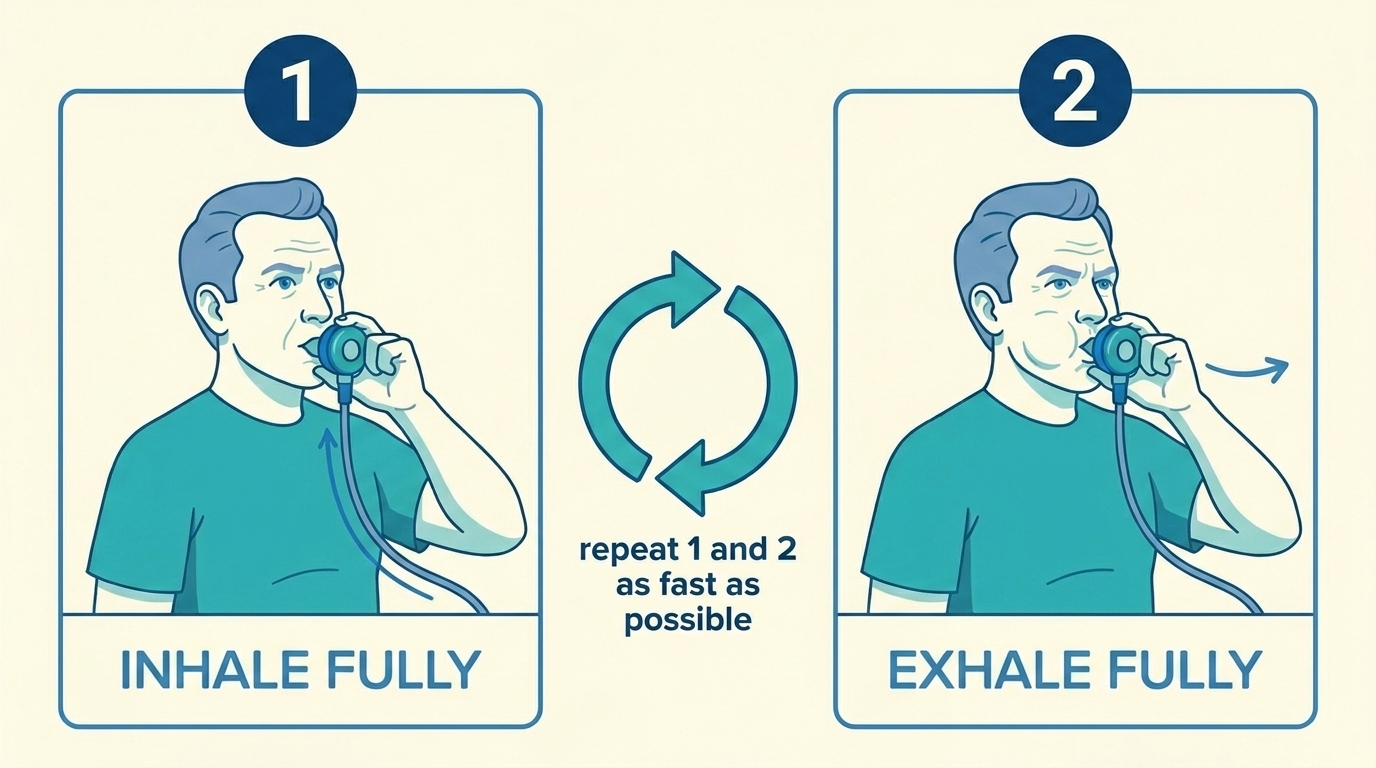 Hyperventilation: inhale fully, exhale fully, repeat as fast as you can.
Hyperventilation: inhale fully, exhale fully, repeat as fast as you can.
Demonstration video of the hyperventilation technique with a demand valve.
Setup
A demand valve is the natural fit, since it releases gas every time you inhale, with no waiting. In a recent patient survey, mean time to a complete abort was about 11 minutes with a demand valve versus 36 minutes with a standard high-flow mask.[2]
You can also hyperventilate on a reservoir bag setup (ClusterO2 kit or non-rebreather mask), but only if your regulator delivers ultra-high flow (typically 40 liters per minute, LPM, or more), so the bag can refill fast enough to keep up with your breathing. Expect to burn through the cylinder quickly.
Deep breathing
The technique
Empty your lungs completely, take a deep inhale of pure oxygen, then exhale fully. Some patients perform an abdominal crunch on the exhale (pulling the belly in hard) to push every last bit of air out. Two sub-techniques, depending on how you chain in- and out-breath cycles:
- No pause: start inhaling immediately after you fully exhale. This is the preferred technique of many patients. Note that it requires a sufficiently high-flow setup. Depending on your lung capacity, you might need 25 LPM, or even more.
- Pause after each inhale. Some patients mentally count until the next exhale. This technique uses less oxygen than the no-pause one, and is the only deep breathing technique available if your setup isn't high-flow enough.
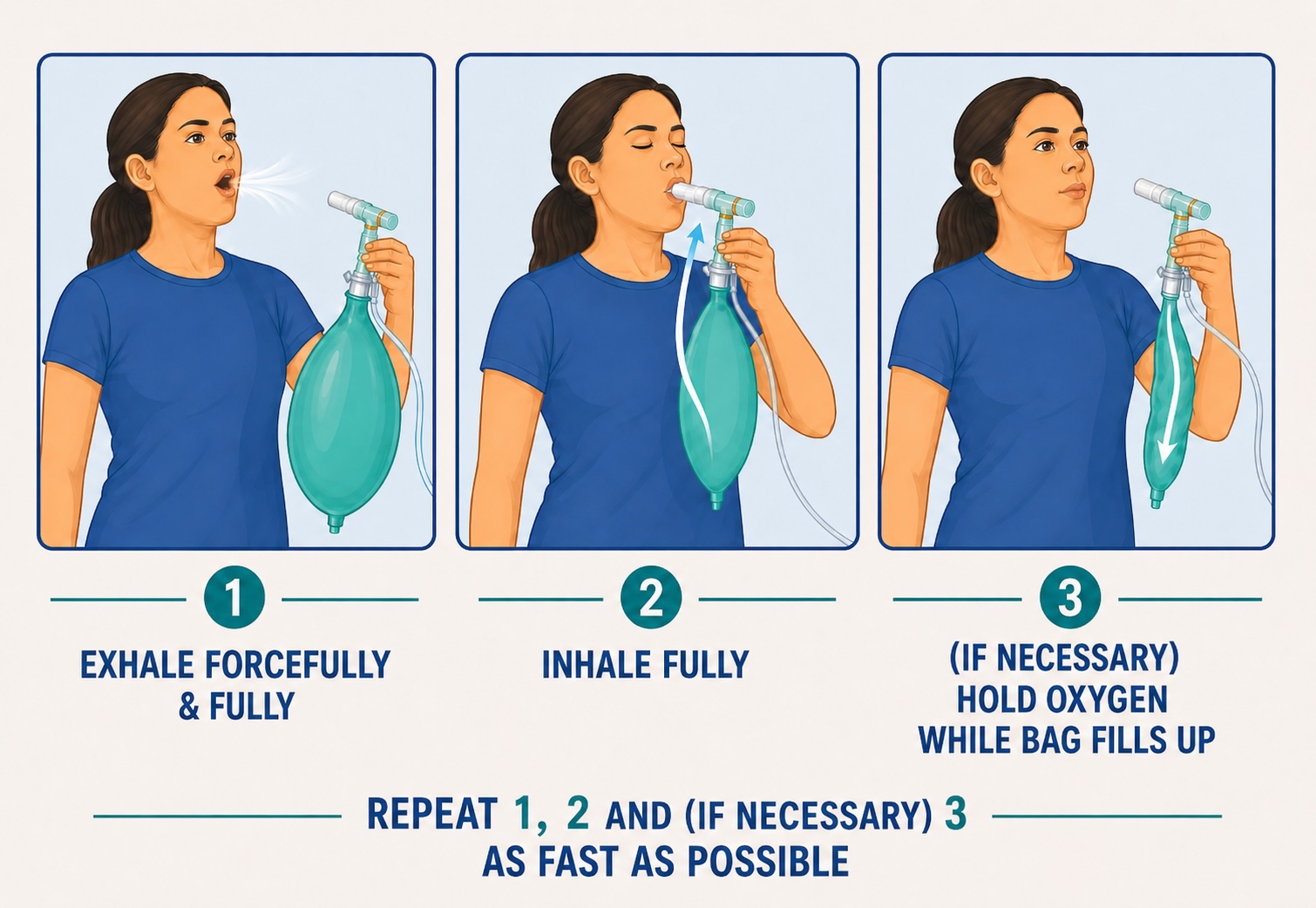 Deep breathing: exhale fully, inhale pure oxygen, and, if needed, hold while the bag refills. Repeat as fast as you can.
Deep breathing: exhale fully, inhale pure oxygen, and, if needed, hold while the bag refills. Repeat as fast as you can.
Demonstration video of the deep breathing technique with a ClusterO2 kit.
How to determine the flow rate. As a starting point, try about 25 LPM for deep breathing and 40 LPM or more for hyperventilation, then adjust from how the bag behaves. Increase the flow if you have to wait more than you'd like for the bag to refill before the next inhale. Decrease the flow, if the bag refills faster than you empty it.
Setup
Deep breathing pairs naturally with a reservoir-bag setup (a ClusterO2 kit or non-rebreather mask). We recommend a flow of at least 25 LPM, and 40 or more is better. If your regulator can't reach that, swap it for a higher-flow one: they are often cheap, suppliers sometimes swap them for free, or your doctor can prescribe one. See the Equipment chapter.
Staying on oxygen after the pain stops
The attack can sometimes restart within minutes. This is rebound, and a few extra minutes of breathing usually prevents it. Our recommendations:
- Stay on oxygen at least 5 minutes after the pain has stopped. Some patients recommend staying on oxygen for at least as long as it took to abort.
- Step the regulator down. Some patients step the regulator down progressively, from 25 LPM to 10, then 8, then 6 over the post-pain window, keeping breathing in and out deeply, but at a slower rhythm. You keep the benefit and use much less gas.
In a 2011 study of patients in modern oxygen practice, only about 4% reported rebound.[3] If you've never had a rebound, you probably won't start having them just because you stopped using oxygen early once. But the 5-minute habit is cheap insurance.
Troubleshooting
Oxygen doesn't always work from the start, and a setup that worked for years can suddenly feel less effective. When it seems to fail, the culprit is almost always equipment, flow, or breathing technique, and all three can be fixed. Before you conclude oxygen isn't working for you, work through the two parts below: first rule out a setup problem, then experiment with your technique.
Troubleshoot your setup
Rule out a setup problem first, since it's usually the quickest thing to fix. Things to check:
- Correct equipment. To abort an attack, the gas you breathe needs to be pure oxygen, undiluted. That means three things to avoid:
- Oxygen concentrators. They produce oxygen at lower purity and at a flow rate too low for cluster aborts. The source gas must come from a pure-oxygen cylinder.
- Nasal cannulas, and masks with open side vents. They let room air mix with the oxygen you inhale. If your prescribed non-rebreather mask has side vents, you can block them. See the Equipment chapter.
- Masks without a reservoir bag. Without a bag to hold a stock of pure oxygen between breaths, the mask cannot deliver enough oxygen on the inhale to completely fill your lungs.
- Mask seal. Hold the mask firmly to your face and check for gaps, especially at the nose bridge. If your mask has side vents or holes, tape them shut or press them closed with your fingers during the session, so room air can't dilute the oxygen. Consider using a mouthpiece (available for instance with the ClusterO2 kit) rather than a mask, held firmly between your lips with a full seal.
- Cylinder pressure. Some patients report oxygen becoming less effective as a cylinder empties. A medical cylinder reads about 2,000 psi (pounds per square inch) when full; below roughly 200 psi the regulator may not keep up with hard, fast breathing. Check the pressure gauge and swap to a fuller cylinder if yours is running low.
- Regulator and flow. Make sure the flow is turned up and the regulator is actually delivering it:
- With a reservoir bag (non-rebreather mask or ClusterO2 kit), the bag should refill between breaths and never fully collapse on inhale, even when you're breathing as fast as you can. If it flattens, turn the flow up.
- With a demand valve, you should hear or feel gas delivered on each inhale. If the valve feels stiff or you're starving for air, check the cylinder, and check that your valve is clean (see just below).
- If using a demand valve, make sure it's paired with a pressure regulator, not a flow (LPM) regulator. See the Equipment chapter.
- Equipment clean, valves working. ClusterO2 kits and demand valves depend on one-way valves. A dirty valve might be stuck. Inspect the valves, confirm they move freely. Clean your breathing equipment with lukewarm water and soap every now and then. Inspect your tubing, mask or mouthpiece, and replace any worn or perished parts.
- Setup properly assembled. Walk through the assembly steps in the Equipment chapter. Two videos are helpful here: a demonstration of the different oxygen setups, and a walkthrough of assembling an OptiMask (a legacy ClusterO2 kit, with a similar design).
Troubleshoot your technique
If the setup checks out, technique is where most of the gains are. No single breathing pattern works for everyone, so this is the thing to experiment with most.
Technique variations to try:
- Breathe deeper and/or faster. Hyperventilation and deep breathing are effortful techniques. If you finished a session without feeling physically tired, there's likely room to push harder.
- Crunch on the exhale. With a deep breathing technique, at the end of each exhale, pull your belly in hard to push out the last residual air sitting at the bottom of your lungs.
- Switch patterns. Experiment with hyperventilation, deep breathing, with and without a pause, and other patterns. See Breathing techniques above.
Other things to try:
- Start earlier. Oxygen works dramatically better when it hits an attack early: earliest aborts often take 3–5 minutes; aborts started at peak pain can take 15–30. Begin at the first hint, even if you aren't sure yet.
- Adjuncts. Pair oxygen with caffeine or cold on the painful side, as described under The abort procedure above.
If you've worked through both parts and oxygen still isn't helping, two further points are worth knowing.
About 1 in 5 patients in trials and large surveys report poor or no response to oxygen.[1] An important caveat: those trials and surveys generally didn't standardize breathing technique. The pivotal 2009 RCT prescribed "12 LPM via non-rebreather for 15 minutes" without instructing patients to hyperventilate, and others have explicitly told participants to "breathe normally." With harder, faster, more sustained breathing, the real non-responder rate is probably lower than the literature suggests. A 2022 review found that poor response is more common among patients who are non-smokers, female (possibly because women have historically been prescribed lower flow rates), with chronic rather than episodic phenotype, longer attacks, or interictal headache between attacks.[4] If you fit several of these, optimizing flow rate and technique tends to give the biggest payoff.
If oxygen reliably makes the pain worse, or never has any effect at all even after careful technique troubleshooting, it's worth asking your specialist whether the diagnosis is right. Hemicrania continua, paroxysmal hemicrania, and trigeminal neuralgia can resemble cluster headache but respond differently. Paroxysmal hemicrania and hemicrania continua are, by definition, indomethacin-responsive, and an indomethacin trial is a standard next step in this situation.
Keeping notes
Oxygen response is personal: the right flow, the right breathing rhythm, the right post-pain duration, the right adjuncts all vary from patient to patient. Tracking your attacks and what you did during each one helps you converge on a routine faster. After an attack, take a minute to write down:
- Your setup and flow (regulator setting, mask or mouthpiece, demand valve or reservoir bag)
- Which breathing technique you used (hyperventilation, or deep breathing with or without a pause)
- How quickly the pain responded, and how long you stayed on after pain-zero
- Any adjuncts (caffeine, cold) and whether they seemed to help
- Anything you'd do differently next time
Over time these notes help you dial in the routine that aborts your attacks fastest. Consider using the free myClusters app, or a simple physical diary.
Conserving oxygen
If you're running short on cylinders, stuck on a low-flow regulator you can't upgrade yet, or just want a tank to stretch further, a few tactics help.
- Hold the inhale. After a full deep inhale of pure oxygen, hold it for one to two seconds before exhaling. More oxygen diffuses across the alveoli per breath, at the cost of slowing the abort somewhat.
- Step the regulator down during the post-pain window. See Staying on oxygen after the pain stops above. Lowering the flow as the pain fades buys most of the rebound-prevention benefit at a fraction of the gas use.
- Try Batch's alternation approach. A community technique developed by Pete Batcheller (a chronic cluster patient, retired Navy pilot, and named inventor on the demand-valve patent) alternates short bursts of hard breathing on room air with held breaths of pure oxygen, on the theory that the room-air phase pre-builds the low-CO₂ part of the abort mechanism without using cylinder gas. The original write-up is on the Clusterbusters "Oxygen stopped to work" thread. This is patient-community evidence rather than trial-tested, and not everyone finds it works for them, but a number of experienced patients use it as their default conservation routine.
Whatever else you change, keep inhaling and exhaling fully. Shallow breaths to save oxygen tend to backfire: the abort drags out and you end up using more gas overall. Fewer, deeper, fuller breaths beat shallower frequent ones.
Safety at home
The same fire-safety rules apply whether your oxygen is medical or welding (no smoking, no oil or grease on fittings, secured upright cylinder, valve closed after every use). See Equipment § Safety at home for the full list.
References
- ↩ Cohen AS, Burns B, Goadsby PJ (2009). High-flow oxygen for treatment of cluster headache: a randomized trial. JAMA, 302(22), 2451–2457. Link
- ↩ Goadsby PJ, et al. (2025). Patient-experience survey comparing high-flow oxygen with demand valve oxygen for cluster headache. Cephalalgia Reports. Link
- ↩ Geerlings RPJ, Haane DYP, Koehler PJ (2011). Rebound following oxygen therapy in cluster headache. Cephalalgia. Link
- ↩ Choi YJ et al. (2022). Oxygen therapy for cluster headache. Journal of Clinical Neurology. Link
Did you find this page helpful?
Disclaimer
The information on this website is provided for educational and harm reduction purposes only. It does not constitute medical advice and should not replace consultation with a qualified healthcare professional. See our Legal page for more details.