Getting a Prescription
What the prescription must say, how to talk to a doctor who isn't familiar with cluster headache, how to navigate insurance and suppliers, and what equipment to insist on.
In the US, UK, EU, Canada, Australia, and most other countries, medical oxygen is a prescription-only medication. Getting the right prescription is the access bottleneck for most patients — and it is routinely the slowest, most frustrating part of the whole journey. The good news: the guidelines are clear, the evidence is strong, and patients who know what to ask for get there faster.
What the prescription must contain
A correct prescription for cluster headache oxygen has six elements:
- 100% oxygen — not blended, not low-concentration.
- Flow rate: ask for the highest the prescriber will write. Aim for 25 L/min. 15 L/min is the bare minimum, not the target. If your prescriber is willing, ask for up to 40 L/min or language like "flow as tolerated" to leave room for ultra-high flow. Do not accept 2–4 L/min (a COPD prescription) or 8–10 L/min.
- Delivery device: non-rebreather mask or demand valve. Not a nasal cannula. Not a simple (Hudson) face mask. Not pulse-dose.
- Use as needed for acute cluster attacks. Without this language, suppliers may ration your oxygen to a fixed schedule.
- Session length: 15–20 minutes per attack. (Sessions up to an hour are safe, so this should not be written as a hard ceiling.)
- Compressed gas cylinders — not an oxygen concentrator. Most concentrators max out around 5–10 L/min and cannot produce the flow rates needed to abort an attack.
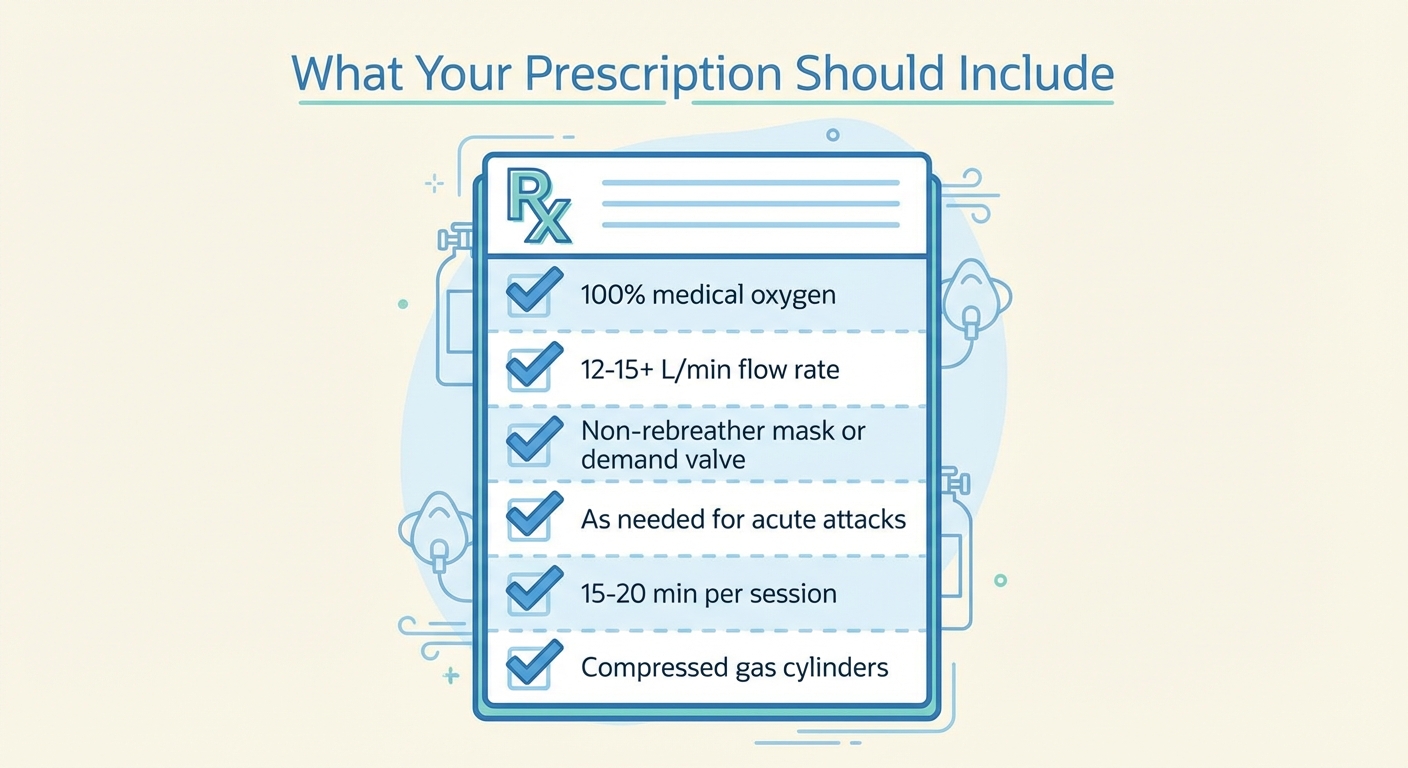 The six elements of a correct prescription. If the illustration shows a 15 L/min flow line, treat that as the floor — ask your prescriber for higher.
The six elements of a correct prescription. If the illustration shows a 15 L/min flow line, treat that as the floor — ask your prescriber for higher.
Common prescription errors to catch
These errors are routine. Read what you're handed before you accept it.
- Flow rate written as the target instead of the floor. A prescription that caps you at 15 L/min leaves you stuck even if you could tolerate and benefit from more. Ask for 25 L/min or "up to 40 L/min as tolerated."
- Nasal cannula. Delivers 25–40% oxygen — not enough to abort an attack. You need a non-rebreather mask or demand valve.
- Oxygen concentrator instead of cylinders. The supplier may prefer this (no refills) but most concentrators can't reach the flow you need.
- Missing "as needed" / PRN language. Can cause the supplier to limit your supply.
- Short session duration (e.g., 10 minutes). Some attacks need 15–20 minutes; the prescription should allow it.
If any of these appear, don't accept the prescription silently. Show your prescriber this checklist and ask for a revision. You're not being difficult — you're preventing weeks of wasted time with equipment that doesn't work.
Talking to a skeptical doctor
Cluster headache affects roughly 1 in 1,000 adults, and oxygen is not routinely taught in medical schools. Many GPs — and a surprising number of neurologists — have never prescribed it. You may need to supply the evidence yourself. These talking points work:
"Oxygen is first-line acute treatment in every major guideline."
- American Headache Society: Level A (highest evidence) recommendation for high-flow oxygen in acute cluster attacks.[1]
- European Academy of Neurology (2023): recommends 100% oxygen via non-rebreather mask at ≥12 L/min as one of only two strongly-recommended acute treatments (the other is subcutaneous sumatriptan).[2]
- NICE (UK): recommends 100% oxygen at a minimum of 12 L/min via non-rebreather mask. Most patients benefit from 15 L/min or higher — patient communities and clinical experience consistently favor higher flows.
"The clinical evidence is strong."
- Cohen et al., JAMA 2009: a double-blind randomized trial of 109 cluster headache patients. 78% of attacks treated with 100% oxygen were pain-free at 15 minutes, compared with 20% on sham air. This is one of the largest treatment effects in acute headache medicine.[3]
- Petersen et al., Cephalalgia 2017: a randomized crossover comparison of demand-valve oxygen vs. standard non-rebreather mask. Demand-valve users needed rescue medication in 23% of attacks vs. 50% with a standard mask, and 62% preferred the demand valve overall.[4]
"It's extremely safe."
- The exposure per session is 15–60 minutes. Oxygen toxicity is a concern at many hours of continuous high-flow breathing, far beyond an abort session.
- No significant adverse events in the Cohen trial or in subsequent reviews.
If your doctor says no
- Ask for a referral to a neurologist or headache specialist. A GP who won't prescribe a Level A, guideline-recommended treatment may simply be outside their comfort zone. A specialist almost always will.
- Bring the printed guidelines. Search for "American Headache Society cluster headache guidelines" and "EAN cluster headache guideline 2023" — both are freely available. Printed guidelines are often more persuasive than a verbal request.
- Switch doctors. This is drastic, but patients consistently report it is sometimes the fastest path. A doctor who dismisses a well-established treatment for a condition this painful is not serving you well.
Insurance and coverage
The system around the prescription is usually harder than the prescription itself.
United States
Medicare coverage for home oxygen for cluster headache improved significantly in 2021, when the previous restriction requiring enrollment in a clinical trial was lifted. Coverage now varies by regional contractor, but the door is open.
Private insurance: many plans cover home oxygen for cluster headache with documentation of medical necessity. Practical steps:
- Check the ICD-10 code on your diagnosis. Cluster headache codes are G44.001 (episodic, intractable), G44.009 (episodic, not intractable), G44.011 (chronic, intractable), and G44.019 (chronic, not intractable). The right code on the paperwork matters.
- Call your insurer directly. Don't rely on the doctor's office or supplier to verify coverage. Call the number on your card and ask: "Is home oxygen therapy covered for cluster headache (ICD-10 G44.0)?"
- If denied, appeal. Include the AHS guideline, the EAN 2023 guideline, and the 2009 JAMA trial. Initial denials are frequently overturned on appeal.
- Ask your doctor to do a peer-to-peer review. A phone call between your doctor and the insurer's medical reviewer is often more effective than written appeals.
- Escalate to your state insurance commissioner if standard appeals fail.
United Kingdom
Oxygen for cluster headache is available through the NHS. The process:
- Get diagnosed by a neurologist or headache specialist.
- Your GP completes a Home Oxygen Order Form (HOOF) — cluster headache is explicitly listed as a qualifying condition.
- A brief home safety assessment (fire risk, smoking status).
- The NHS oxygen supplier (typically BOC or Baywater, depending on your region) delivers the equipment.
If your GP hesitates, point them to the HOOF form (which lists cluster headache), the British National Formulary entry for oxygen, and NICE guidance. Demand valves are available on the NHS for chronic cluster headache patients; episodic patients can typically rent one from BOC.
Elsewhere
Most European and Commonwealth countries cover oxygen for cluster headache through their national systems, but the process varies. The general shape is the same: diagnosis from a specialist → prescription → supplier assignment. Ask your neurologist's office who handles medical oxygen in your region, and whether they've prescribed it for cluster headache before.
If your country makes medical oxygen genuinely inaccessible, welding oxygen is a well-established alternative used by a sizable share of patients worldwide.
Working with suppliers
Once the prescription is written, it's routed to an oxygen supplier — a durable medical equipment (DME) company in the US, the NHS contractor in the UK, or a regional equivalent elsewhere. You can usually choose between suppliers; some are noticeably better than others.
What to ask a supplier before you commit:
- "Do you carry regulators that go to 25 L/min or higher?" If the answer is no, pick a different supplier or plan to buy your own regulator separately.
- "Can you deliver a demand valve?" (More likely in the UK and at larger US suppliers.)
- "What's your emergency or weekend refill process?" Cluster cycles don't stop on Friday at 5pm.
- "How often will you refill cylinders during an active cycle?" Some suppliers cap delivery frequency in ways that don't match cluster usage.
Common supplier problems and how to handle them:
- They try to send an 8 L/min regulator (designed for COPD patients). Decline. Insist on ≥25 L/min, or buy your own — a high-flow oxygen regulator runs $30–80 online and is a one-time cost.
- They try to substitute a concentrator for cylinders. Politely decline. Your prescription specifies compressed gas. If they push back, have your doctor call them.
- Refill delays during a cycle. Always keep at least one full backup cylinder. Track your usage and call for refills before the primary runs low, not after. Ask about larger cylinder sizes if the refill cadence can't keep up.
Equipment: what to insist on
Your supplier delivers three things (sometimes four): a cylinder, a regulator, a delivery device (mask or demand valve), and tubing. What to insist on:
- A regulator that goes to at least 25 L/min. Decline an 8 L/min (COPD) regulator. If the supplier can't provide a high-flow one, you can buy one online for $30–80.
- Compressed gas cylinders, not a concentrator. Most concentrators max out around 5–10 L/min and can't reach abort flow rates.
- A demand valve if it's available on your plan (more likely on the NHS and at larger US suppliers). A ClusterO2 kit or non-rebreather mask is a reasonable fallback.
- An outlet on the regulator that matches your delivery device — barb for standard tubing-to-mask setups, DISS for most demand valves.
For detail on each piece of equipment — how demand valves, masks, regulators, and cylinders actually work and which differences matter — see the Equipment chapter.
If you can't get a prescription
If insurance and supplier routes fail — or your region makes medical oxygen genuinely hard to access — there are alternatives:
- Pay out of pocket for medical oxygen. A DME supplier will usually deliver to a self-pay patient once a prescription is on file; the process is often faster than insurance coverage. Monthly cost runs $200–400 in the US.
- Welding oxygen. The same O₂ molecule, sold without a prescription at welding supply shops, at a fraction of the medical cost. A well-researched option used by a sizable share of patients, with the same safety considerations as medical oxygen. See the dedicated page: Welding oxygen: a practical alternative.
- Oxygen concentrators do not require a prescription in many countries. They can't match compressed-gas flow rates and are not adequate as a primary setup — but partial flow is better than nothing, and some patients use one as a backup.
References
- ↩ American Headache Society (2021). The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice. Headache. Link
- ↩ European Academy of Neurology (2023). European Academy of Neurology guideline on the treatment of cluster headache. European Journal of Neurology. Link
- ↩ Cohen AS, Burns B, Goadsby PJ (2009). High-flow oxygen for treatment of cluster headache: a randomized trial. JAMA, 302(22), 2451–2457. Link
- ↩ Petersen AS, Barloese MCJ, Lund NLT, Jensen RH (2017). Oxygen therapy for cluster headache. A mask comparison trial. A single-blinded, placebo-controlled, crossover study. Cephalalgia, 37(3), 214–224. Link
¿Te ha resultado útil esta página?
Descargo de Responsabilidad
La información en este sitio web se proporciona únicamente con fines educativos y de reducción de daños. No constituye asesoramiento médico y no debe reemplazar la consulta con un profesional de salud calificado. Consulte nuestra página de Aviso Legal para más detalles.