Aborting an Attack with Oxygen
How to use oxygen during a cluster attack. Technique matters more than equipment; equipment matters more than dose. Underdo any of the three and oxygen can feel like it doesn't work.
The single most common reason oxygen "fails" isn't bad oxygen, bad equipment, or the wrong patient. It's under-breathing. Oxygen is a physical treatment: you have to move a lot of it into your lungs, fast, for it to shut down an attack. This page is about doing that correctly.
The breathing technique (read this first)
Inhale as deeply as your lungs will allow. Exhale completely: forcefully push as much air out as you can. Repeat this deep-inhale-and-exhale cycle as fast as you can.
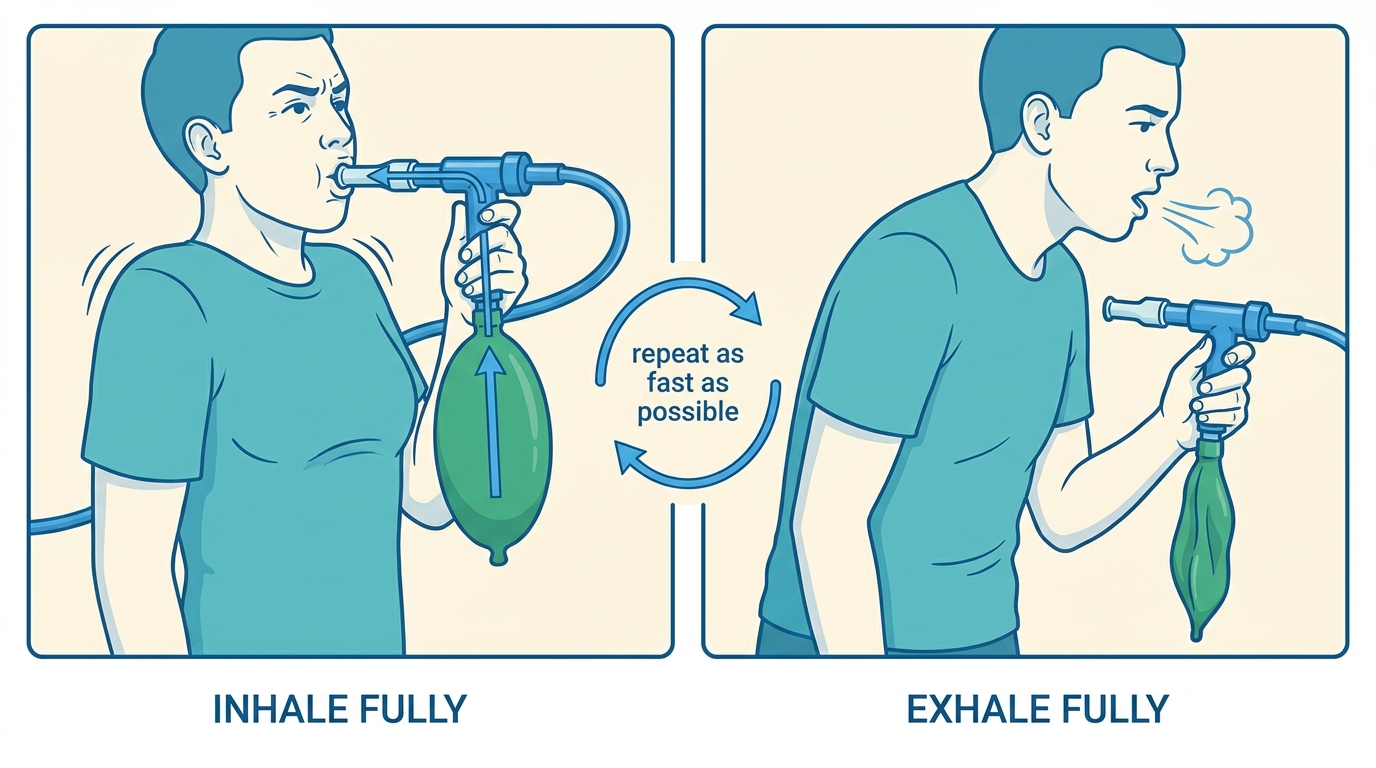 Inhale fully, exhale fully, repeat as fast as you can — the same cycle applies whether you're breathing through a mouthpiece or a sealed mask.
Inhale fully, exhale fully, repeat as fast as you can — the same cycle applies whether you're breathing through a mouthpiece or a sealed mask.
This breathing technique requires high- or even ultra-high-flow oxygen: we recommend a setup that can output at least 25 liters per minute (LPM). That also means that it consumes a lot of oxygen. If you don't have access to a high-flow setup, or want to preserve oxygen, check out the "If you can't get a high LPM setup" section below.
A few things to understand about it:
- It's effortful. You are working. Your chest and shoulders should be moving hard. If you finish a 10-minute session without feeling physically tired, you probably weren't breathing hard enough.
- Breathing fast matters. There is evidence that the faster you complete each full inhale-exhale cycle, the faster and more effective the abort.
- Start as early as you can. Oxygen works dramatically better when it hits an attack early. Start as soon as you feel warning signs, don't wait until you're sure.
- Try a crunch on the exhale. Some patients recommend pulling your belly in hard at the end of the exhale: an abdominal "crunch". This pushes out the last CO₂-rich air sitting at the bottom of your lungs. It also makes the next inhale of pure oxygen go deeper. Some experienced patients found this adjustment to significantly shorten their abort time.
- Light-headedness, tingling sensations or numbness are normal. Those are normal and benign side-effects of hyperventilation. It is actually a good sign: it means you're breathing hard enough.
Some patients start with an all-out sprint for 2–3 minutes, then settle into a slightly steadier rhythm once the pain begins to ease. Others stay aggressive the whole way. Try both and see what your body responds to.
Adjusting your setup while breathing
What you watch during the session depends on your delivery equipment:
- Demand valve. The valve opens when you inhale and closes when you don't; there's nothing to adjust mid-attack. You should hear/feel gas delivered on each inhale. If the valve feels stiff or you're starving for air, check the cylinder has pressure.
- Reservoir bag (non-rebreather mask or ClusterO2 kit with bag). The bag should refill between breaths and never fully collapse when you inhale, even when you're breathing as fast as you can. If it flattens, turn the flow up.
- Non-rebreather mask with side vents. The small open holes or valves on the sides of the mask can let room air in and dilute your oxygen. We recommend to press them shut with your fingers.
- Mouthpiece. Hold it firmly between your lips with a full seal.
The abort procedure
This procedure works for any setup: demand valve or reservoir-bag, mask or mouthpiece.
- At the first sign of an attack, get to your oxygen.
- Sit upright. Many patients find leaning forward slightly on elbows or a table helps; experiment.
- Open the cylinder valve (counter-clockwise on top) and set the regulator to its highest flow.
- Put on your mask or mouthpiece and start breathing: inhale and exhale fully, and as fast as you can. (See "Breathing technique" above.)
- Keep going until the pain is completely gone (not just reduced). Typical relief comes in 5–15 minutes. Longer sessions (under an hour) are safe and sometimes necessary.
- Stay on for at least 5 minutes after the pain is gone. Stopping the moment pain eases is a common way to trigger a bounce-back within minutes.
- Close the cylinder valve and ventilate the room. Don't smoke or produce sparks until the room is well-aired.
If it's not working
Oxygen therapy is notoriously difficult to get right. It can also work for you for a while and suddenly become less effective. The most important advice in such cases is: Don't give up. Experiment.
If it's not working well enough for you, here are a few things to consider:
- Are you breathing hard and fast enough? Try pushing harder.
- Did you start early enough? Next time, start at the first hint.
- Is your flow high enough? If the flow is limiting how quickly you can take oxygen in: increase it if your setup allows it. If your setup doesn't allow you to increase the flow, consider changing it. If you can't, check the section just below for tips on aborting with little oxygen.
- If you have a mask: is the seal tight? Hold it firmly against your face, and check there are no gaps at the nose bridge. If side valves or holes are present, try blocking them with your fingers. Finally, consider using a mouthpiece instead of a mask.
- Is the cylinder actually delivering gas? Check pressure; a cylinder under ~200 PSI may not deliver enough flow under load.
If you can't get a high LPM setup, or if you need to conserve oxygen
The breathing technique described above is thought to be the most efficient at aborting. It will unfortunately require at least 25 LPM for a person with typical lung capacity, and will consume a lot of oxygen.
If you don't have access to a high LPM setup, or need to preserve your oxygen, here are things you can try:
- Hold the oxygen in. Some patients hold the full inhale for a second or two (some silently count) before exhaling.
- Hyperventilate on room air first. Some patients suggest hyperventilating (forcefully breathing in and out as quickly as possible) on room air, before switching to pure oxygen. They report needing less pure oxygen that way. You can check out a video demonstration here.
Whatever you do, focus on inhaling and exhaling fully. It might be tempting to draw shallow breaths to preserve oxygen. Do not do that: evidence suggests that fully filling and emptying the lungs matters a lot.
Safety at home
Fire-safety rules (no smoking, no oil or grease on fittings, secured upright cylinder, valve closed after every use) apply to every oxygen setup, medical or welding. See Equipment § Safety at home for the full list.
War diese Seite hilfreich?
Haftungsausschluss
Die Informationen auf dieser Website dienen ausschließlich Bildungszwecken und der Schadensminimierung. Sie stellen keine medizinische Beratung dar und sollten nicht die Konsultation einer qualifizierten medizinischen Fachkraft ersetzen. Weitere Einzelheiten finden Sie auf unserer Seite Rechtliche Hinweise .